Related Subjects:
|ECG Basics
|ECG Axis
|ECG Analysis
|ECG LAD
|ECG RAD
|ECG Low voltage
|ECG Pathological Q waves
|ECG ST/T wave changes
|ECG LBBB
|ECG RBBB
|ECG short PR
|ECG Heart Block
|ECG Asystole and P wave asystole
|ECG QRS complex
|ECG ST segment
|ECG: QT interval
|ECG: LVH
|ECG RVH
|ECG: Bundle branch blocks
|ECG Dominant R wave in V1
|ECG Acute Coronary Syndrome
|ECG Crib sheets
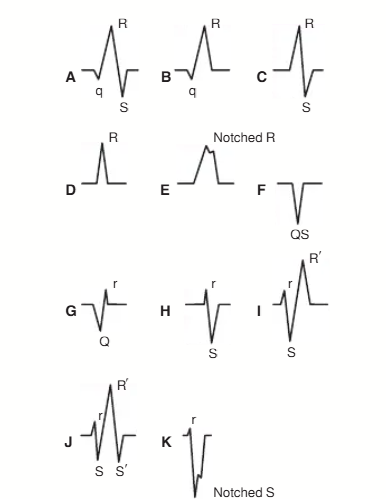
📌 About the QRS Complex
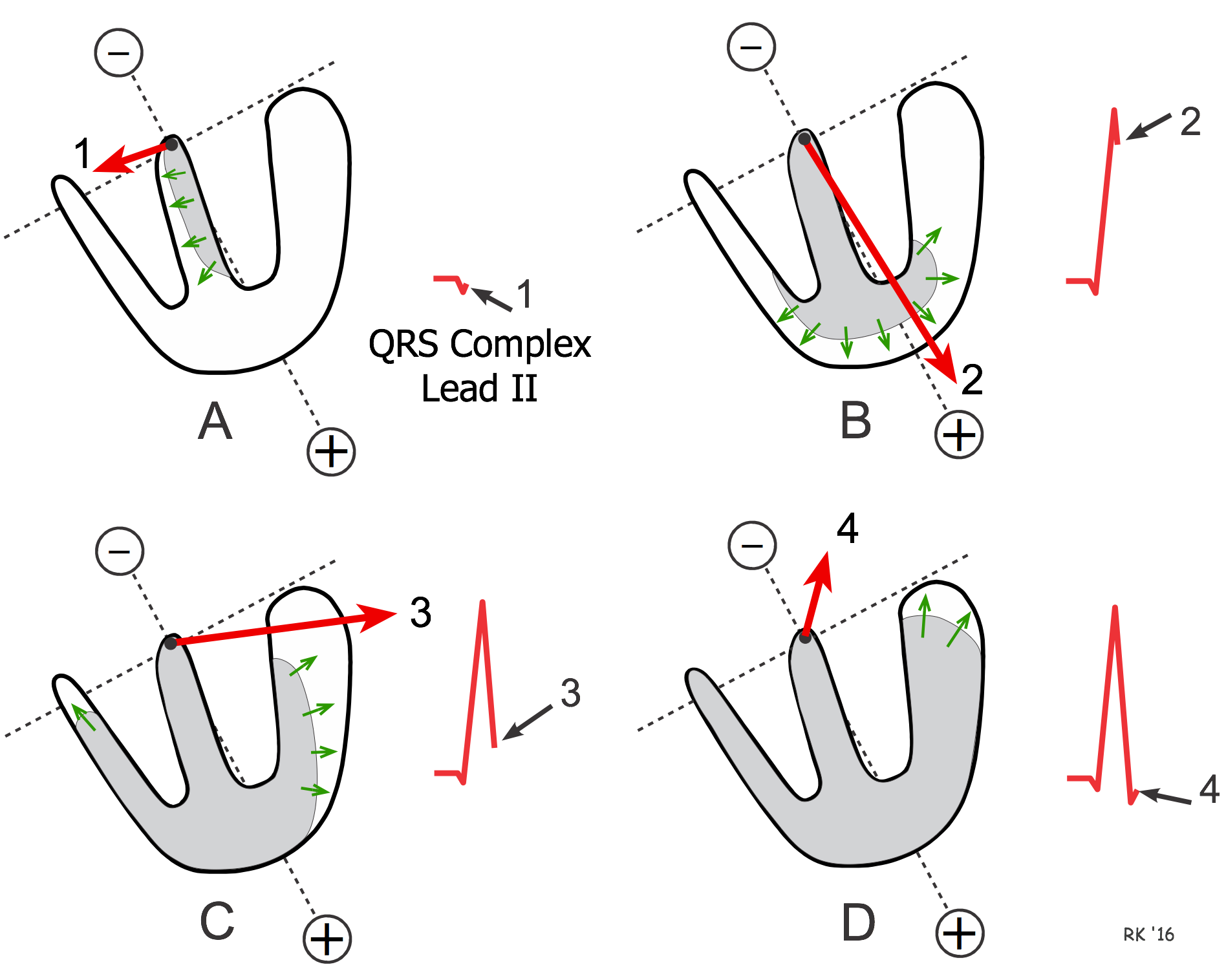
- The QRS complex is the surface ECG recording of ventricular depolarisation.
- Any surface ECG lead records the net sum of voltages in that view of the heart.
- Depolarisation begins in the AV node → spreads into the interventricular septum (left side first, then right side).
- The left ventricle forms the bulk of the depolarising muscle, hence dominates the QRS signal.
- Depolarisation moves through Purkinje fibres from endocardium → myocardium → epicardium.
- Left-sided leads (I, aVL, V4–V6): small initial Q wave (septal depolarisation away) → large R wave (towards apex of LV).
- Right-sided leads (V1, V2): small r wave (septum) → deep S wave (depolarisation away).
- Normal QRS duration: <120 ms (3 small squares).
📐 QRS Axis
- Represents the net direction of ventricular depolarisation.
- Calculated using limb leads (I and aVF at 90° to each other).
- Normal axis: –30° to +90°.
- Right Axis Deviation (>+90°): Right ventricular hypertrophy (RVH), left posterior fascicular block.
- Left Axis Deviation (<–30°): Left ventricular hypertrophy (LVH), left anterior fascicular block.
💪 Left Ventricular Hypertrophy (LVH)
- Axis shifts leftward; increased voltage in left-sided leads (I, II, aVL, V5, V6).
- ECG criteria: S in V1 + R in V5/6 >35 mm, or R in aVL >11 mm.
- Strain pattern may develop: ST depression & T wave inversion in left leads.
- Chronic LVH can progress to LBBB.
💪 Right Ventricular Hypertrophy (RVH)
- Increased voltage in right-sided leads (V1, V2), often dominant R in V1.
- Left-sided leads usually unchanged.
- May see right atrial enlargement; with time → RBBB.
⚡ Bundle Branch Blocks
- LBBB: RSR′ in V6; RV depolarises first → then delayed LV.
- RBBB: RSR′ in V1; LV depolarises first → then delayed RV.
📊 Wide QRS (>0.12s)
- Conduction defects: LBBB, RBBB.
- Ventricular origin of complex (e.g. VT).
- Pre-excitation: Wolff-Parkinson-White (delta wave).
- Electrolyte abnormality: Hyperkalaemia (broad, slurred QRS).
⬆️ Increased QRS Voltage
- LVH: S in V1 + R in V5/6 >35 mm.
- RVH: Dominant R wave in V1.
- Hypertrophic cardiomyopathy.
⬇️ Decreased QRS Voltage
- Obesity, pericardial effusion.
- Hypothyroidism, emphysema (increased thoracic impedance).
🚑 Red Flags
- New LBBB + chest pain: Treat as STEMI equivalent. → 999 call, O₂, nitrates, aspirin.
- Regular broad-complex tachycardia >120 bpm: Assume Ventricular Tachycardia until proven otherwise → urgent hospital referral.
