Related Subjects:
|Hyperkalaemia
|ECG - Hyperkalaemia
|Hypokalemia
|Hyperkalaemic and Hypokalaemic Periodic Paralysis
|Resuscitation - Advanced Life Support
|Action Potential
⚡ Hyperkalaemia is a medical emergency because it can trigger fatal arrhythmias, muscle weakness, paralysis, and cardiac arrest.
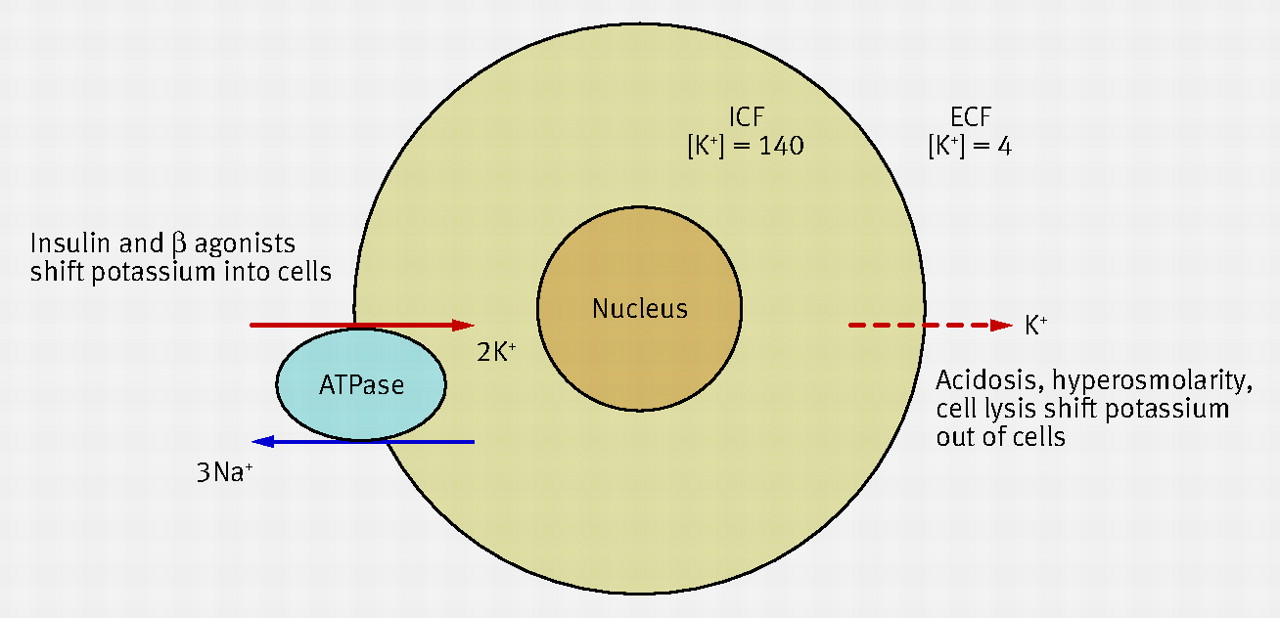
Rising extracellular K⁺ partially depolarises the resting membrane potential, which inactivates fast Na⁺ channels and slows conduction through myocardium and skeletal muscle.
💉 Calcium gluconate is often preferred for peripheral administration because it is less irritant than calcium chloride, but remember: calcium stabilises the myocardium - it does not lower serum potassium.
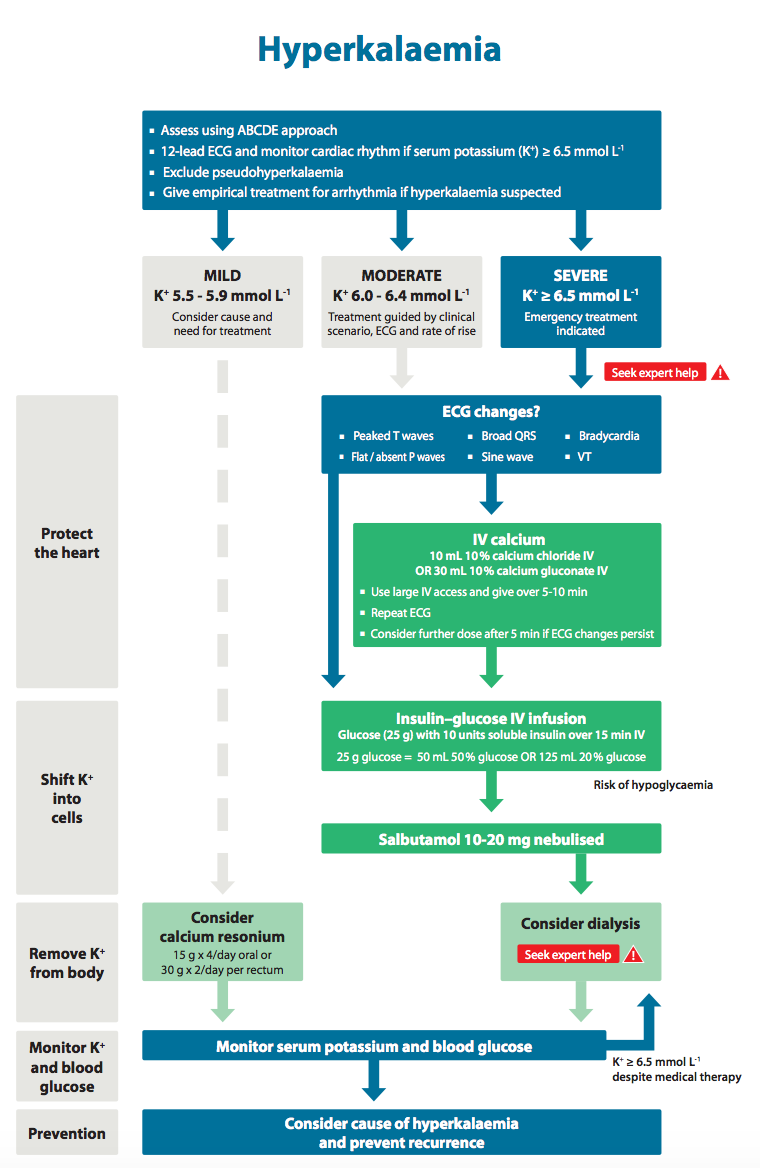
| 🚑 Emergency Management: Severe Hyperkalaemia |
- 📟 Continuous ECG monitoring, urgent ECG, IV access, repeat potassium urgently if the result is unexpected or haemolysis is suspected.
- 💉 If ECG changes are present: give 10% calcium gluconate IV or 10% calcium chloride IV slowly; repeat if ECG changes persist.
- 💉 Shift K⁺ into cells: 10 units soluble insulin + 25 g glucose IV.
- 🍬 Monitor capillary glucose closely after insulin; give follow-on glucose according to blood glucose and local protocol.
- 🌬️ Salbutamol 10–20 mg nebulised as an adjunct.
- 💊 Sodium zirconium cyclosilicate (Lokelma) may be added as an adjunct in acute hyperkalaemia, but it is not a substitute for immediate emergency treatment.
- 💧 Stop potassium-raising drugs and treat the underlying cause.
- 💧 Consider IV fluids if hypovolaemic; consider a loop diuretic only if volume status and renal function make it appropriate.
- 🩺 Arrange urgent dialysis if hyperkalaemia is refractory, recurrent, or associated with advanced renal failure / missed dialysis.
- 💉 Sodium bicarbonate may be considered if there is significant metabolic acidosis, especially in peri-arrest or arrest settings.
|
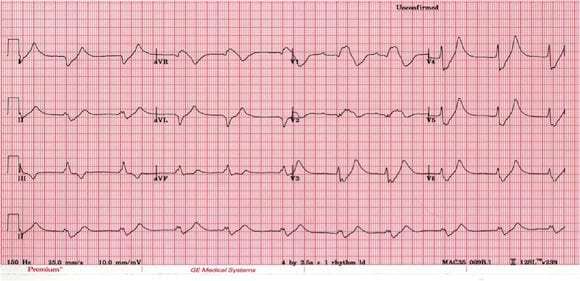
📉 ECG Changes (Act Fast!)
- ⚠️ Typical progression: tall peaked T waves → PR prolongation → flattening/loss of P waves → QRS widening → sine-wave pattern → VT/VF / asystole
- ⚠️ ECG changes are not perfectly reliable: some patients with severe hyperkalaemia have surprisingly subtle ECG changes, while others deteriorate quickly.
🧠 Physiology
- High extracellular K⁺ reduces the transmembrane gradient and partially depolarises excitable cells.
- This causes inactivation of fast Na⁺ channels, so conduction becomes slower and action potentials become less effective.
- That is why hyperkalaemia causes bradycardia, conduction block, broad QRS complexes, muscle weakness, and eventually arrest.
- 💉 IV calcium counteracts the membrane instability and buys time, but it does not remove potassium from the body.
📋 Aetiology (Always Check the Drug Chart)
- 🩺 AKI / CKD, missed dialysis
- 💊 Drugs: ACE inhibitors, ARBs, spironolactone, eplerenone, amiloride, NSAIDs, trimethoprim, heparin, ciclosporin / tacrolimus
- 🧬 Endocrine / renal tubular causes: Addison’s disease, type 4 RTA
- 🩸 Cell breakdown: rhabdomyolysis, trauma, burns, tumour lysis, haemolysis
- 🧪 Acidosis (especially DKA)
- 🍫 Excess potassium intake / salt substitutes can contribute, especially when renal excretion is impaired
- ⚠️ Pseudohyperkalaemia: haemolysed sample, fist clenching, prolonged tourniquet use, marked thrombocytosis / leukocytosis, lab error
🧾 Clinical Features
- Often asymptomatic until severe
- 💪 Weakness, cramps, paraesthesia, ascending flaccid weakness
- 🫀 Palpitations, bradycardia, syncope, hypotension
- 🚨 Arrhythmia or cardiac arrest may be the first presentation
📊 Severity
- Mild: 5.5–5.9 mmol/L
- Moderate: 6.0–6.4 mmol/L
- Severe: ≥6.5 mmol/L
- 🚑 Treat urgently if K⁺ is severe, or if K⁺ is >6.0 mmol/L with ECG changes, rapid rise, or the patient is clinically unwell.
🔬 Investigations
- Repeat potassium urgently if the result is unexpected or haemolysis is possible.
- U&E, creatinine, bicarbonate, calcium, magnesium
- VBG / ABG if acidosis or severe illness is suspected
- FBC if infection, haemolysis, thrombocytosis, or haematological cause is suspected
- CK if rhabdomyolysis is possible
- ECG in all significant hyperkalaemia
⚕️ Management Summary
- 1️⃣ Protect the heart: IV calcium if ECG changes
- 2️⃣ Shift potassium intracellularly: insulin + glucose, plus nebulised salbutamol
- 3️⃣ Remove potassium from the body: stop exogenous potassium, consider potassium binders, loop diuretics if suitable, and dialysis if needed
- 4️⃣ Treat the cause: AKI, DKA, missed dialysis, rhabdomyolysis, drugs, acidosis, adrenal disease
- 5️⃣ Monitor closely: serial potassium checks, serial glucose after insulin, and continuous ECG monitoring in severe cases
💔 Hyperkalaemia in Cardiac Arrest / Peri-Arrest
- Think of hyperkalaemia in renal failure, missed dialysis, crush injury, rhabdomyolysis, DKA, or patients on potassium-raising drugs.
- 💉 Give IV calcium urgently to stabilise the myocardium.
- 💉 Give 10 units soluble insulin + 25 g glucose IV.
- 🌬️ Give nebulised salbutamol 10–20 mg.
- 💉 Consider 50 mmol sodium bicarbonate if there is marked metabolic acidosis.
- 🩺 Arrange urgent dialysis if refractory or in severe renal failure.
- ⚠️ Potassium often rebounds after initial treatment, so ongoing reassessment is essential.
📚 References
- UK Kidney Association. Management of Hyperkalaemia in Adults (2023).
- Resuscitation Council UK. 2025 Resuscitation Guidelines – Special circumstances: hyperkalaemia.
- BNF / NICE. Hyperkalaemia – treatment summary.
- NICE TA599. Sodium zirconium cyclosilicate for treating hyperkalaemia.
Cases - Hyperkalaemia
- Case 1: A 68-year-old man with CKD stage 4 and poorly controlled hypertension presents with weakness. ECG shows tall peaked T waves. Serum potassium is 6.8 mmol/L.
Management: IV calcium to stabilise the myocardium, insulin/glucose, nebulised salbutamol, hold ramipril, consider sodium zirconium cyclosilicate as an adjunct, and monitor potassium plus glucose closely.
Outcome: Potassium falls over several hours and he avoids dialysis.
- Case 2: A 42-year-old man with type 1 diabetes presents in DKA with potassium 7.2 mmol/L. ECG shows absent P waves and widened QRS.
Management: IV calcium, insulin therapy with glucose strategy as needed, aggressive fluid resuscitation, DKA treatment, and close cardiac monitoring.
Outcome: As acidosis resolves, potassium falls and later careful potassium replacement becomes necessary.
- Case 3: A 79-year-old woman taking spironolactone and an ACE inhibitor presents collapsed, bradycardic, and hypotensive. Potassium is 8.1 mmol/L and the ECG shows a sine-wave pattern.
Management: Immediate IV calcium, insulin/glucose, nebulised salbutamol, stop potassium-raising drugs, correct acidosis if present, and arrange emergency dialysis.
Outcome: She survives after critical care and medication review.
Teaching Commentary 🧑⚕️
Hyperkalaemia kills by disrupting cardiac excitability and conduction, not simply because the potassium number is high. The management logic is therefore sequential: first stabilise the myocardium, then shift potassium into cells, then remove potassium from the body, while urgently treating the underlying cause. One subtle but important practical point is that insulin therapy can save a life but also cause dangerous hypoglycaemia, which is why serial glucose monitoring and follow-on glucose are so important. Another high-yield nuance is that ECG changes are helpful but imperfect - never be falsely reassured by a near-normal tracing in a patient with a very high potassium and the right clinical context.
