
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Malaria Falciparum (Cerebral Malaria) ✅
Related Subjects: |Fever in a traveller |Malaria Falciparum (Cerebral Malaria) |Malaria |Malaria in Children |Viral Haemorrhagic Fevers (VHF) |Lassa fever |Dengue |Marburg virus disease |AIDS HIV |Yellow fever |Ebola Virus |Leptospirosis |Crimean-Congo haemorrhagic fever |African Trypanosomiasis (Sleeping sickness) |American Trypanosomiasis (Chagas Disease) |Incubation Periods |Notifiable Diseases UK
⚠️ Always consider malaria in anyone with fever or a flu-like illness who has travelled to, lived in, or migrated from a malaria-risk area - even up to 1 year after return. 👉 Falciparum malaria is a medical emergency: patients can deteriorate rapidly and die before the post-take ward round. 🧪 Send urgent thick and thin blood films plus malaria antigen testing, inform the laboratory, and involve Infectious Diseases / Tropical Medicine early. ❗ A single negative film does not exclude malaria - repeat testing is required if clinical suspicion remains. Management: Artesunate is first-line for severe malaria, quinine is the fallback if artesunate is not available, doxycycline should be avoided in pregnancy, and “treat bacterial co-infection” is softened to consider and cover if clinically suspected or severely unwell.
| 🚑 Initial Management – Severe / Complicated Malaria (Notifiable) |
|---|
|
📖 About
- Falciparum malaria is the most lethal form and may deteriorate rapidly without treatment.
- Parasitaemia >2% is high-risk and should prompt urgent specialist review; >5% is a poor prognostic feature and suggests severe disease.
- BNF Malaria Treatment Summary
🦟 Vector & Parasite
- Spread by the female Anopheles mosquito.
- Caused by the protozoan parasite Plasmodium falciparum.
- Other routes: transfusion, needlestick, “airport malaria” (imported mosquitoes).

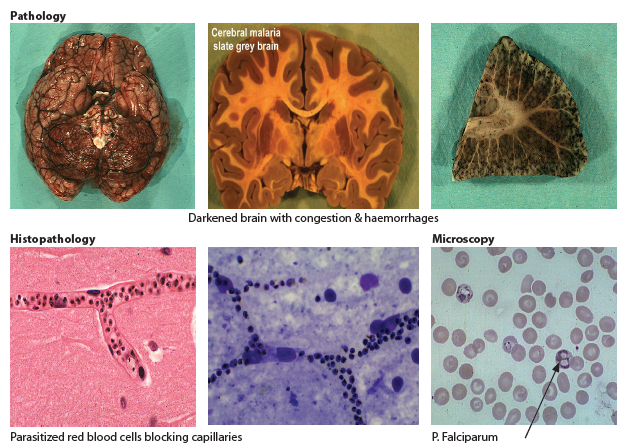
🧬 Pathophysiology
- Cytoadherence: Infected RBCs stick to endothelium → block venules.
- Mediated by PfEMP-1 on red cell surface.
- Leads to cerebral, renal, pulmonary, and multi-organ damage.
- Rosetting: Infected cells clump with normal RBCs, worsening occlusion.
🌍 Epidemiology
- Malaria causes hundreds of thousands of deaths globally each year, with the highest burden in sub-Saharan Africa.
- Endemic areas include sub-Saharan Africa, parts of Asia, Oceania, Central and South America, and the Caribbean.
- In the UK, malaria is usually an imported infection and is a notifiable disease.
🔄 Life Cycle (Simplified)
- 🦟 Mosquito bite → sporozoites enter liver.
- 🩸 Liver stage → merozoites released into blood.
- RBC stage → multiplication and rupture of RBCs (rigors, fever, anaemia).
- Adherence to endothelium → organ damage (brain, kidney, lung, gut).
🩺 Clinical Features
- Malaise, fatigue, fever, delirium, diarrhoea and abdominal pain
- Flu-like illness: fever, malaise, headache, rigors.
- Hepatosplenomegaly (mild).
- Severe: cerebral malaria → coma, seizures, hemiparesis, blindness.
- Exposure (Foreign travel) within < 1-6 months
⚠️ Complications
- Coma, seizures (reduced GCS).
- Acute renal failure (10% need dialysis).
- Metabolic acidosis, hypoglycaemia (from parasite + quinine).
- Severe anaemia, haemolysis, jaundice.
- “Blackwater fever” (haemoglobinuria).
- DIC, thrombocytopenia.
- ARDS / non-cardiogenic pulmonary oedema.
⚠️ Severity
- Uncomplicated: parasitaemia <2%, no schizonts, no clinical complications
- Severe: parasitaemia >2%, or schizonts/complications even if <2%
🧪 Investigations
- Bloods: FBC, U&E, LFTs, glucose, lactate, blood cultures.
- Films: 3–5 thick & thin blood films over 48 hrs. Thick = parasite detection, Thin = speciation + parasitaemia %.
- Parasitaemia >5% or pre-schizont forms → poor prognosis.
- Rapid antigen detection (useful in UK hospitals).
- Other: CXR (pneumonia), urinalysis, stool culture, COVID test if relevant.
🔎 Differentials (coinfection possible!)
- Dengue, Typhoid, Schistosomiasis, Tick typhus.
- TB, Dysentery, Influenza, Viral or bacterial pneumonia.
- HIV, bacterial sepsis, meningitis.
💊 Management (BNF-linked)
- 🟢 Uncomplicated falciparum malaria (oral treatment):
- Discuss all confirmed or suspected malaria cases with Infectious Diseases / Tropical Medicine.
- Options include artemether-lumefantrine, atovaquone-proguanil, or quinine plus doxycycline.
- If using quinine: give quinine for 5–7 days plus doxycycline for 7 days.
- Use clindamycin instead of doxycycline in pregnancy or where doxycycline is contraindicated.
- Choice depends on species, severity, pregnancy status, drug interactions, resistance risk, previous prophylaxis and specialist advice.
- 🔴 Severe / complicated falciparum malaria:
- Medical emergency: ABCDE, admit to HDU/ICU, involve ID/Tropical Medicine urgently, and inform the laboratory.
- Monitor glucose frequently, as severe malaria and quinine can both cause hypoglycaemia.
- Use careful fluid balance - avoid both dehydration and fluid overload / ARDS.
- First-line: IV Artesunate 2.4 mg/kg at 0, 12 and 24 hours, then OD until able to switch to oral therapy. Once improving and able to swallow, complete treatment with an appropriate full oral antimalarial course as advised by specialists.
- Second-Line: IV quinine may be considered if IV artesunate is not immediately available:. IV quinine regimen: loading dose 20 mg/kg, then 10 mg/kg every 8 hours; avoid loading dose if quinine, quinidine or mefloquine has recently been given. With quinine: check ECG/QTc, monitor for arrhythmias, hypotension and hypoglycaemia.
- Correct hypoglycaemia, treat seizures according to local status epilepticus guidance, transfuse if severe anaemia, and manage renal failure/acidosis with critical care input.
- Consider bacterial sepsis/co-infection; take cultures and give broad-spectrum antibiotics if clinically suspected or the patient is severely unwell, but do not delay antimalarial treatment.
- 🤰 Pregnancy:
- Malaria in pregnancy is high risk, especially falciparum malaria, because of increased risk of severe disease, hypoglycaemia, anaemia, fetal loss, preterm birth and maternal death.
- All pregnant patients with suspected malaria need urgent specialist input from Infectious Diseases / Tropical Medicine and Obstetrics.
- Uncomplicated falciparum malaria: quinine plus clindamycin is commonly used; avoid doxycycline in pregnancy.
- Severe / complicated malaria: treat as a medical emergency - IV artesunate is generally preferred; IV quinine is an alternative if artesunate is not available.
- Monitor glucose closely, as both pregnancy and severe malaria increase the risk of hypoglycaemia.
📞 UK Expert Advice
- PHE Malaria Reference Laboratory: 020 7637 0248
- NaTHNaC: 0845 602 6712
- HPS Travax (Scotland): www.travax.nhs.uk
- Regional Centres: Birmingham, Liverpool, London, Oxford
Cases - Malaria (Plasmodium falciparum)
- Case 1 - Uncomplicated Malaria in a Traveller: A 27-year-old man returns from Nigeria with fever, chills, sweats, and headache 10 days after travel. He did not take prophylaxis. Exam: febrile, mild jaundice, splenomegaly. Blood film: parasitaemia 2% with ring forms. Diagnosis: Uncomplicated falciparum malaria. Management: Oral artemisinin-based combination therapy (artemether-lumefantrine) if able to tolerate orally; admit for monitoring.
- Case 2 - Severe Malaria with Cerebral Involvement: A 34-year-old woman presents after returning from India with confusion, seizures, and fever. Exam: GCS 9, splenomegaly. Bloods: Hb 7.5 g/dL, lactate raised, parasitaemia 8%. Diagnosis: Severe falciparum malaria with cerebral involvement. Management: Admit to ICU. IV artesunate (first-line) or IV quinine if unavailable, supportive care for seizures and hypoglycaemia, careful fluid balance.
- Case 3 - Malaria in Pregnancy: A 22-year-old woman at 26 weeks’ gestation, recently returned from Ghana, presents with fever, myalgia, and vomiting. Exam: febrile, tachycardic, mild hepatosplenomegaly. Blood film confirms falciparum malaria, parasitaemia 4%. Diagnosis: Falciparum malaria in pregnancy. Management: IV artesunate if severe; if uncomplicated and able to tolerate oral therapy: artemisinin-based combination therapy (artemether-lumefantrine) or quinine + clindamycin (depending on gestation and national guidelines). Urgent obstetric + infectious disease review.
Teaching Commentary 🦟
*P. falciparum* is the most dangerous malaria species due to its ability to cause high parasitaemia, microvascular sequestration, and multi-organ dysfunction. - Uncomplicated malaria: fever, sweats, headache, splenomegaly - treat with oral ACT. - Severe malaria: cerebral features, acidosis, renal failure, shock, high parasitaemia - treat with IV artesunate. - Pregnancy: higher risk of severe disease, miscarriage, and low birth weight. Key principles: confirm diagnosis with thick and thin blood films (or rapid antigen tests), admit all falciparum malaria cases initially, and escalate to ICU if severe.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery