Related Subjects:
|Breast Anatomy and Examination (OSCE)
|Shoulder examination(OSCE)
|Breast Anatomy and Examination (OSCE)
|Shoulder examination(OSCE)
|Testicular examination(OSCE)
|Hernia Examination (OSCE)
|Rectal examination (OSCE)
|Liver Examination (OSCE)
|Cerebellar Examination (OSCE)
|Upper and Lower Limb Neurology (OSCE)
|Gastroenterology Examination (OSCE)
|Respiratory Examination (OSCE)
|Cardiology Examination (OSCE)
|OSCE Eye Exam
|OSCE Ear Exam
|OSCE Abdominal Exam
|OSCE Ascites Exam
|OSCE Jaundice Exam
|OSCE Testicular Exam
|OSCE Inguinal Exam
|OSCE Upper limb Neurology
|OSCE Lower limb Neurology
|OSCE Face Neurology
|OSCE Visual Fields
Raised Blood Pressure Consultation & Accurate Measurement – OSCE Guide – Updated Feb 2026
💉 Raised BP consultation = **from door handle to documented plan**.
This guide covers: structured history, **gold-standard BP measurement technique**, red flags, investigations, risk assessment, shared decision-making, and safety-netting.
Key principle: Accurate BP measurement is the foundation - poor technique = wrong diagnosis = wrong treatment.
1️⃣ Before You See the Patient (Pre-consult Prep – 1–2 min)
- 📄 Check record: previous BP readings (clinic/ABPM/HBPM), HTN diagnosis date, current meds (adherence, side effects), target organ damage (LVH on ECG, proteinuria, retinopathy), CKD (eGFR), diabetes, lipids, QRISK3 score if available.
- ⚠️ Scan for red flags: recent chest pain/SOB/neuro symptoms, very high BP (≥180/120), end-organ damage (papilloedema, encephalopathy, acute kidney injury), secondary causes clues (young age, resistant HTN, hypokalaemia).
- 🧠 Frame your aims: “Is this true sustained hypertension? Any target organ damage? What’s the 10-year CV risk? Lifestyle first or meds? Can we realistically improve this?”
2️⃣ Opening the Consultation (1–2 min)
- 👋 Introduce & identify: “Hello, I’m Dr X, one of the doctors here. Could I confirm your full name and date of birth?”
- 🗣️ Reason for visit: “I see you’ve come about your blood pressure today. Can you tell me what’s been happening?”
- 📋 Agenda setting: “Today I’d like to hear your story, check your blood pressure properly (using the correct technique), look at risk factors, and agree a plan together. Does that sound OK?”
- ICE (Ideas, Concerns, Expectations): “What do you think might be causing it? Anything you’re particularly worried about (e.g., stroke, heart attack)? What were you hoping we could do today?”
3️⃣ Focused History for Raised BP (3–5 min)
- Presenting issue:
- “How was high BP picked up?” (routine GP check, workplace screening, pharmacy, home monitor, A&E, pre-op).
- “Have you had more than one reading? Do you remember the numbers?”
- “Any symptoms?” – headaches (occipital, morning), visual changes (blurring, scotoma), chest pain/tightness, dyspnoea, palpitations, epistaxis, polyuria/nocturia (DM/CKD), neurological (TIA/stroke symptoms).
- Cardiovascular & renal symptoms:
- Exertional chest pain, breathlessness, orthopnoea, PND, ankle swelling (HF).
- Neurological: TIAs, strokes, focal weakness, speech disturbance, confusion (hypertensive encephalopathy).
- Renal: frothy urine (proteinuria), haematuria, nocturia, loin pain.
- Past medical history:
- Known HTN (date diagnosed, previous control), CKD, diabetes, hyperlipidaemia, AF, IHD, HF, stroke/TIA, PVD.
- Secondary causes clues: young-onset (<40), resistant HTN (>3 drugs), hypokalaemia (primary aldosteronism), snoring/apnoeas (OSA), Cushingoid features, acromegaly.
- Drug history:
- Current antihypertensives (adherence, side effects: cough – ACEi, ankle oedema – CCB, gout – diuretics, fatigue – beta-blockers).
- Other meds: NSAIDs, COCP/HRT, decongestants, steroids, stimulants, herbal remedies (liquorice, ephedra), chemotherapy.
- Allergies/intolerances (e.g., ACEi angioedema).
- Family history:
- Premature MI/stroke (<55 men, <65 women), familial hypercholesterolaemia, polycystic kidneys, endocrine disease (phaeochromocytoma, MEN).
- Lifestyle & risk factors:
- Smoking/vaping (pack-years), alcohol (units/week), recreational drugs (cocaine, amphetamines – hypertensive crisis).
- Diet (salt intake, processed foods), caffeine, weight changes (recent gain/loss).
- Physical activity (sedentary vs active), sleep (snoring, witnessed apnoeas, non-restorative sleep – OSA), stress (work, life events).
4️⃣ Accurate Blood Pressure Measurement – Gold-Standard Technique (2–3 min)
💉 Correct technique is heavily marked - poor method = invalid reading = wrong diagnosis.
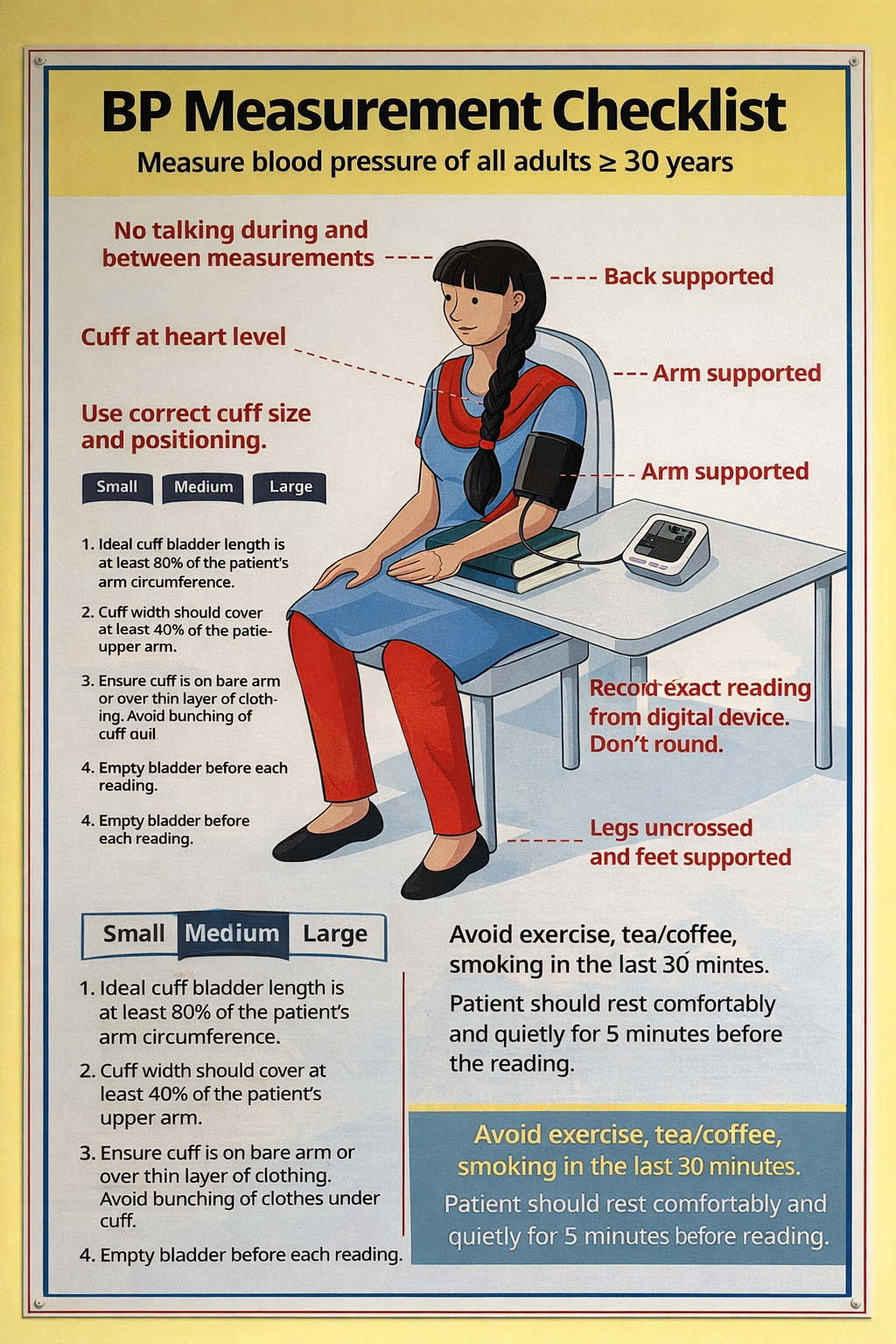
- 🧘 Patient preparation:
- Seat quietly for ≥5 minutes before measurement.
- Feet flat on floor, legs uncrossed, back supported, arm supported at heart level (no talking, no phone).
- No caffeine, exercise, or smoking for 30 min prior.
- 🩹 Cuff selection & placement:
- Use correct cuff size: bladder encircles ≥80% of arm (small cuff → falsely high; large → falsely low).
- Centre bladder over brachial artery (medial to biceps tendon), lower edge 2–3 cm above antecubital fossa.
- Secure firmly but not tight.
- ✋ Estimate systolic pressure (palpatory method):
- Palpate brachial or radial artery.
- Inflate cuff until pulse disappears → note pressure (estimated systolic).
- Deflate fully, wait ≥30 s before auscultation.
- 🎧 Auscultatory measurement (Korotkoff method):
- Place stethoscope bell/diaphragm over brachial artery (not under cuff edge).
- Inflate 20–30 mmHg above estimated systolic.
- Deflate slowly (~2 mmHg/s), listen for Korotkoff phases:
- Phase I: first clear tapping = systolic BP
- Phase V: complete disappearance = diastolic BP
- If sounds persist to zero (pregnancy, hyperdynamic states) use Phase IV (muffling) as diastolic.
- 📝 Recording & interpretation:
- Take ≥2 readings ≥30 s apart; average them. If differ by >10 mmHg, take additional and average last two.
- Measure both arms at first visit (use higher arm for future); difference >15–20 mmHg → investigate (subclavian stenosis, dissection).
- Record: systolic/diastolic, arm used, cuff size, position, device (manual/automated), time of day.
📊 NICE 2026 BP Thresholds & Definitions
| Category | Clinic BP | ABPM/HBPM Daytime Average | Action |
|---|
| Normal | <140/90 | <135/85 | Monitor if risk factors |
| Stage 1 HTN | 140–159 / 90–99 | 135–149 / 85–94 | Treat if <80y + target organ damage, CVD, renal disease, diabetes, or QRISK3 ≥10% |
| Stage 2 HTN | 160–179 / 100–109 | 150–179 / 95–109 | Treat |
| Severe HTN | ≥180/≥120 | - | Urgent same-day review/treatment |
🚩 Red Flags & Secondary HTN Clues
- Urgent referral (same day): BP ≥180/120 + symptoms (headache, visual disturbance, chest pain, dyspnoea, confusion) → hypertensive emergency.
- Secondary HTN clues:
- Young age (<40) or resistant HTN (>3 drugs)
- Hypokalaemia + metabolic alkalosis → primary aldosteronism
- Snoring/apnoeas → OSA
- Radio-femoral delay → coarctation
- Abdominal bruit → renal artery stenosis
- Cushingoid features → Cushing’s syndrome
🔍 General Examination (2–3 min)
- Vitals: BP both arms, HR/rhythm, RR, O₂ sats, temperature, BMI.
- Cardiovascular: collapsing pulse (AR), slow-rising (AS), JVP (fluid overload), displaced apex (LVH), murmurs (aortic valve disease), peripheral oedema.
- Fundoscopy (if able): AV nipping, cotton wool spots, haemorrhages, papilloedema (malignant HTN).
- Abdominal: aortic aneurysm (expansile mass), renal bruits (renal artery stenosis).
- Peripheral vasculature: peripheral pulses, bruits, ankle–brachial index if PVD suspected.
📈 Investigations After the Consultation
- Confirm diagnosis: ABPM (preferred) or HBPM (if ABPM declined/intolerant).
- ABPM: daytime average ≥135/85 = HTN.
- HBPM: average of 7 days (discard day 1) ≥135/85 = HTN.
- Baseline bloods: U&Es, eGFR, electrolytes (hypokalaemia → aldosteronism), lipids, HbA1c, FBC, LFTs, TFTs (if indicated).
- Urine: dipstick (protein/haematuria), ACR (CKD screening).
- ECG: LVH (voltage criteria), prior MI, AF, conduction disease.
- Others if indicated: Echocardiogram (LVH, valve disease), renal ultrasound (renal artery stenosis, polycystic kidneys), renin/aldosterone ratio (secondary HTN), sleep study (OSA).
🍏 Lifestyle & Medication Plan (Shared Decision-Making)
- Lifestyle (first-line for Stage 1 + low risk):
- Weight loss: 5–10% → 5–20 mmHg drop.
- Salt reduction: <6 g/day → 4–5 mmHg drop.
- Alcohol: ≤14 units/week → 3–4 mmHg drop.
- Exercise: 30 min aerobic most days → 4–9 mmHg drop.
- DASH diet, smoking cessation, stress reduction.
- Medication (NICE 2026 algorithm):
- <40y or Black African/Caribbean → start ACEi/ARB + CCB.
- >55y or not Black African/Caribbean → start CCB or thiazide-like diuretic.
- Step 2: ACEi/ARB + CCB or thiazide.
- Step 3: ACEi/ARB + CCB + thiazide.
- Resistant HTN → add spironolactone (if K⁺ normal) or alpha/beta-blocker.
🔟 Safety-Netting & Follow-Up
- Arrange follow-up: 4–12 weeks depending on severity (sooner if severe HTN or organ damage).
- Urgent review if: chest pain, SOB, new neuro deficit, visual loss, severe headache, BP ≥180/120 with symptoms.
- Provide written info/app links (e.g., Blood Pressure UK, NHS BP app).
- Teach home monitoring technique if starting HBPM.
📌 OSCE & Viva Exam Tips
- Always mention: correct cuff size, 5 min rest, no talking, both arms, averaging readings, Korotkoff phases.
- In AF: “I would take multiple readings due to beat-to-beat variability and average them.”
- Remember pulse pressure findings (AS, AR), arm–arm differences (>15–20 mmHg → investigate).
- Close with clear plan: “We’ll confirm with ABPM/HBPM, check bloods and ECG, calculate QRISK3, and then decide together on lifestyle and medication.”
📚 References (Feb 2026)
- NICE NG136 Hypertension in adults (updated 2026).
- British and Irish Hypertension Society – BP Measurement Guidelines (2025).
- QRISK3 Calculator (2025 version).
- Recent: ABPM vs HBPM meta-analysis (Lancet 2025), resistant HTN workup (J Hypertens 2026).
