
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Superior Vena Caval Obstruction syndrome
Related Subjects: |Hypercalcaemia |Neutropenic Sepsis |Pulmonary Embolism |Lung Cancer |Superior vena caval obstruction syndrome |Cerebral Metastases |Metastatic bone disease |Oncological emergencies
🚨 Superior vena cava (SVC) obstruction develops in 5–10% of patients with right-sided malignant intrathoracic mass lesions. ⚡ Early recognition and treatment are crucial to prevent life-threatening complications.
📖 About
- Superior Vena Cava (SVC) Obstruction: Blockage of venous return from the head, neck, arms, and upper chest to the heart.
- 🫁 Usually due to external compression or intraluminal thrombosis.
- 🧑⚕️ Recognised as an oncological emergency in clinical practice.
🧬 Aetiology
- 🚫 Impedes venous return → ↑ venous pressure in upper body.
- 🧩 SVC has thin walls and low pressure → easily compressed by mediastinal structures.
- 📍 Location: lies adjacent to right upper lobe and mediastinum → vulnerable to compression by tumours.
- ~85% of cases = malignancy (lung cancer, lymphoma).
⚠️ Causes
- Malignancy: NSCLC, SCLC, lymphoma, metastatic disease.
- Thrombosis: Related to CVCs, pacemakers, or PICC lines.
- Fibrosis: Mediastinal fibrosis post-infection or radiotherapy.
- Vascular: Aortic aneurysm, AV fistula.
- Infections: TB, syphilis, histoplasmosis.
- Children: Non-Hodgkin’s lymphoma is a common cause.
🩺 Clinical Features
- 😶🌫️ Facial/neck swelling, plethora, dyspnoea, persistent cough.
- 🫁 Severe: stridor, wheeze, airway compromise (tracheal compression).
- 🧵 Dilated neck & chest wall veins (collaterals).
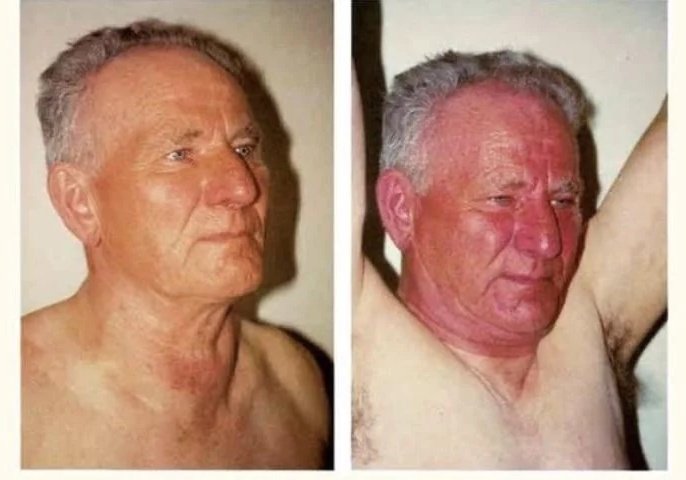
- 🙆♂️ Pemberton’s sign: Raising arms above head → facial congestion & cyanosis worsens.
🔬 Investigations
- Bloods: FBC, U&E, LFTs, CRP, calcium, ALP.
- CXR: Widened mediastinum; ± right pleural effusion (~25%).
- CT Chest: Gold standard – defines site, cause, biopsy planning.
- Sputum Cytology: May identify lung malignancy.
- Contrast Venography: Definitive but invasive – rarely required if CT sufficient.
🧪 Pathology
- 🔴 Majority = malignancy (lung ca, lymphoma).
- Either direct invasion or external compression of SVC wall.
💊 Management
- Supportive: ABC, oxygen, elevate head, secure airway if threatened.
- Steroids: May reduce swelling, esp. with lymphoma.
- Radiotherapy: Treatment of choice for NSCLC.
- Chemotherapy: Effective in SCLC and lymphoma.
- Venous Stenting: Rapid palliation; used if recurrent or severe obstruction.
- Thrombosis: Remove causative line/device, start anticoagulation.
📌 UK Exam Pearls
- 🚨 SVC obstruction is an oncological emergency → urgent oncology input needed.
- 🫁 Most common cause = lung cancer (esp. right-sided). In children → lymphoma.
- 🙆♂️ Pemberton’s sign is highly testable and a classic finding.
- ⚡ Stenting provides the fastest symptomatic relief, especially if airway/brain perfusion threatened.
- 📍 Distinguish malignant vs thrombotic cause → treatment strategy differs.
🚩 SVC Obstruction Red Flags:
- 🧠 Raised ICP: headache, confusion, papilloedema.
- 🫁 Airway compromise: stridor, severe dyspnoea.
- 👁️ Rapidly progressive facial/neck swelling with cyanosis.
- ⚡ Syncope or cardiovascular compromise.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery