
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Artery of Percheron stroke
Related Subjects: |Acute Stroke Assessment (ROSIER&NIHSS) |Atrial Fibrillation |Atrial Myxoma |Causes of Stroke |Ischaemic Stroke |Cancer and Stroke |Cardioembolic stroke |CT Basics for Stroke |Endocarditis and Stroke |Haemorrhagic Stroke |Stroke Thrombolysis |Hyperacute Stroke Care
🧠 Artery of Percheron (AOP) is a rare vascular variant where a single perforating artery supplies both paramedian thalami (± midbrain). This is unusual because most cerebral arteries respect the midline.
📖 About
- First described in 1973 by French neurologist Gérard Percheron.
- Supplies bilateral paramedian thalami (≈30% of cases).
- Important cause of acute coma with otherwise normal early CT.
⚙️ Pathophysiology
- Occlusion → bilateral medial thalamic infarcts ± midbrain involvement.
- 🛌 Classic triad: altered mental status, vertical gaze palsy, memory disturbance.
- Coma occurs due to involvement of the thalamic–reticular activating system.
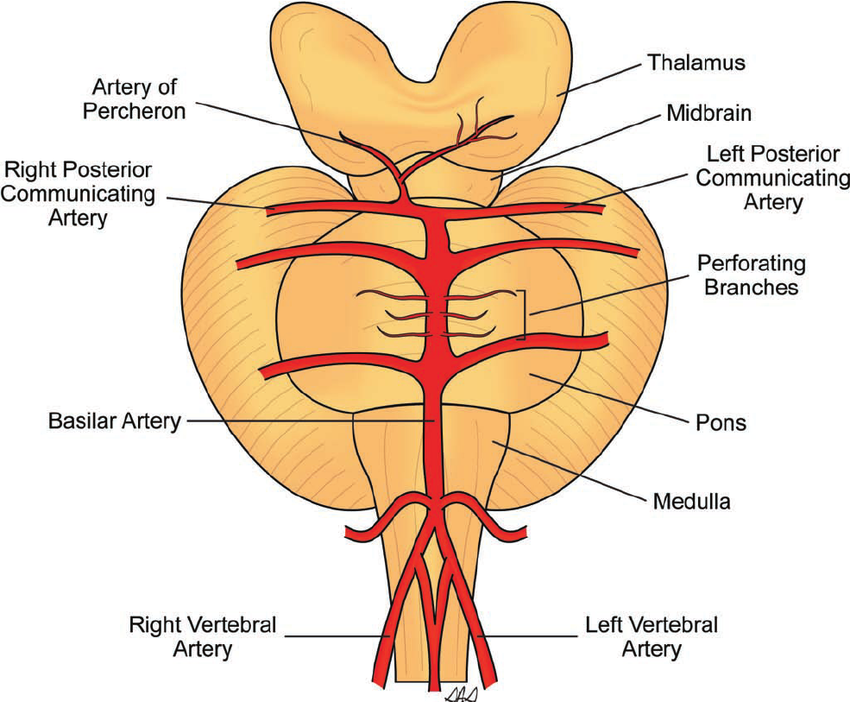
🧩 Anatomy
- Usually, each medial thalamus has its own arterial supply.
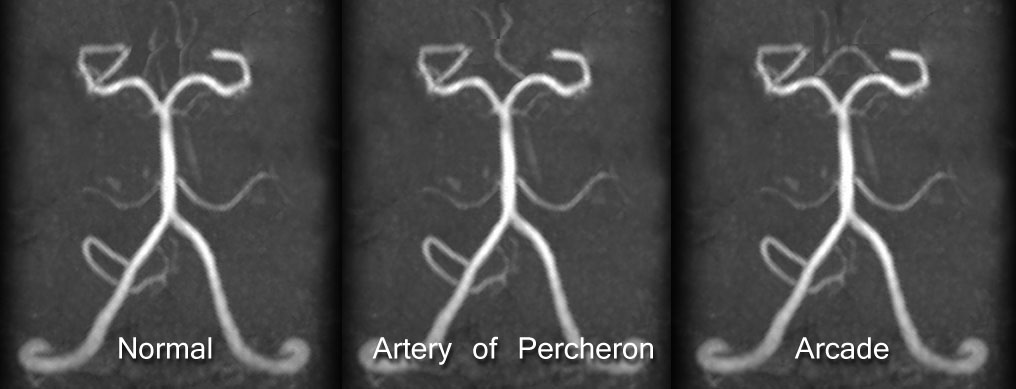
- AOP arises from a single P1/P2 segment of the PCA → bifurcates to supply both thalami.
- Common error: It comes from the PCA, not the posterior communicating artery.
📊 Epidemiology
- Rare: 0.1–2% of all ischaemic strokes.
- A typical UK stroke centre (~1,000 cases/yr) may see only 1–2 cases annually.
🧬 Aetiology
- Cardioembolic (AF, LV thrombus) or artery-to-artery embolism.
- Less common: vertebral artery dissection.
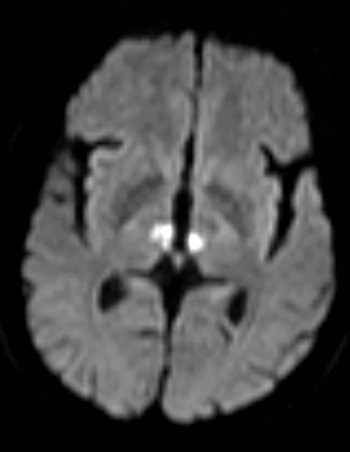
🧲 MRI Appearance
- 🎯 “Butterfly sign”: bilateral paramedian thalamic infarcts.
- 🪶 “V sign” in interpeduncular fossa (seen in ~67%).

🩺 Clinical Presentation
- Acute coma 🛌 or profound somnolence.
- Vertical gaze palsy 👀 and pupillary abnormalities (± pinpoint pupils).
- ⚡ Memory/cognitive deficits often persist.
- If midbrain involved → hemiplegia or CN III palsy.
🔑 Mnemonic: AOP → “3 C’s”: Coma, Cognition, Cranial nerve palsy.
🔍 Differentials (Coma with normal CT)
- Meningoencephalitis 🦠
- Opiate/sedative overdose 💊
- Pontine stroke 🧠
- Post-ictal state ⚡
- Hypoglycaemia 🍬
🧪 Investigations
- Bloods: FBC, U&E, CRP, ESR, cholesterol.
- Cardiac: ECG + Holter, echo (look for AF or thrombus).
- CT: often normal early; later → thalamic hypodensity.
- MRI DWI: diagnostic (butterfly/V-sign).
- CTA/MRA: may show vertebral dissection.
- LP: usually normal, rules out infection.
💊 Management
- Immediate ABC support.
- Thrombolysis/thrombectomy if within window (rarely achieved due to delayed Dx).
- If diagnosis uncertain → treat empirically for infection until confirmed.
- Standard secondary prevention: antiplatelets, BP control, statins.
- Neurorehab + neuropsychology for cognitive recovery.
📌 Exam Pearl: “Coma + normal CT” → always think of Artery of Percheron infarct as a differential.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery