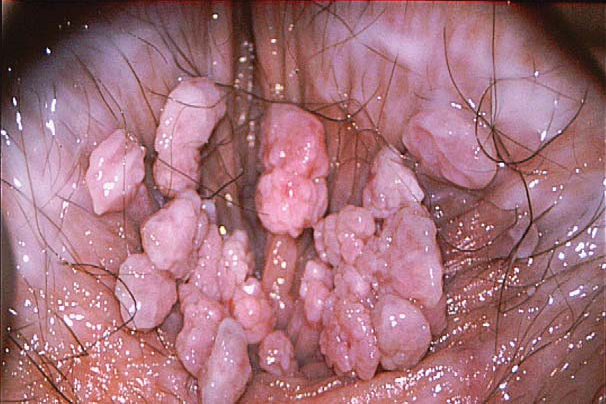
Anogenital Warts (HPV) ✅
🧠 Anogenital warts are common, benign epithelial lesions caused most often by low-risk HPV.
They can be psychologically distressing, but they are not usually dangerous.
Symptoms may appear weeks to many months after infection, so they are not a reliable marker of recent exposure.
🦠 Cause
- HPV types 6 and 11 🌿 cause most typical anogenital warts and have low oncogenic risk.
- Transmission 🤝 is mainly by skin-to-skin sexual contact. HPV may be passed on even when no visible warts are present.
- Condoms 🛡️ reduce transmission risk but do not eliminate it, because uncovered skin can still transmit HPV.
- High-risk HPV types (for example 16/18) ⚠️ are associated with dysplasia and cancer risk, but they do not usually cause typical visible warts.
🔍 Diagnosis
- Clinical diagnosis 👀 is usually sufficient based on typical appearance.
- Biopsy 🔬 should be considered if the diagnosis is uncertain, or if lesions are atypical (for example pigmented, indurated, fixed, ulcerated, bleeding, or suspicious for malignancy).
- HPV testing 🧾 is not used for diagnosing warts.
- Consider differential diagnoses such as molluscum contagiosum, pearly penile papules, papillomatosis vulvae, condylomata lata, skin tags, intraepithelial neoplasia, and malignancy.
💊 Treatment Options
- Patient-applied 🧴: podophyllotoxin or imiquimod may be used for suitable external lesions; both can cause local irritation.
- Clinician-applied ❄️: cryotherapy is commonly used, often requiring repeated sessions.
- Procedural ✂️: excision, electrosurgery, or laser may be used for large, resistant, keratinised, or obstructive lesions.
- Treatment choice 🎯 depends on site, size, number, keratinisation, access, pregnancy status, and patient preference. There is no single “best” treatment for all warts.
- HPV vaccination 💉 helps reduce the risk of future HPV-related disease, but it does not treat existing warts.
🤰 Pregnancy
- If pregnant, referral to a sexual health specialist is usually appropriate.
- Many topical creams/liquids/ointments used for wart treatment are not recommended in pregnancy.
- Warts in pregnancy are often managed conservatively unless they are troublesome, very large, or causing obstruction.
📣 Practical Counselling
- Recurrence is common 🔁 and reflects HPV persistence, not necessarily treatment failure.
- Partners ❤️ may already have HPV even if asymptomatic; partner notification is usually pragmatic and symptom-led rather than formal contact tracing.
- Advise re-attendance if lesions change, bleed, ulcerate, become painful, or fail to respond to treatment.
- People eligible for cervical screening should continue screening as normal.
- Safer sex measures and avoiding sex while lesions are being treated may help reduce onward spread.