Related Subjects:
|AIDS (HIV) Neurological Disease
|AIDS (HIV) Respiratory disease
|AIDS Dementia Complex (HIV)
|AIDS HIV Infection
|AIDS(HIV) Gastrointestinal Disease
|Acute Retroviral Syndrome (HIV)
|HIV and Post-Exposure Prophylaxis (PEP)
|HIV and Pre-exposure prophylaxis
|HIV associated nephropathy (HIVAN)
|HIV disease Assessment
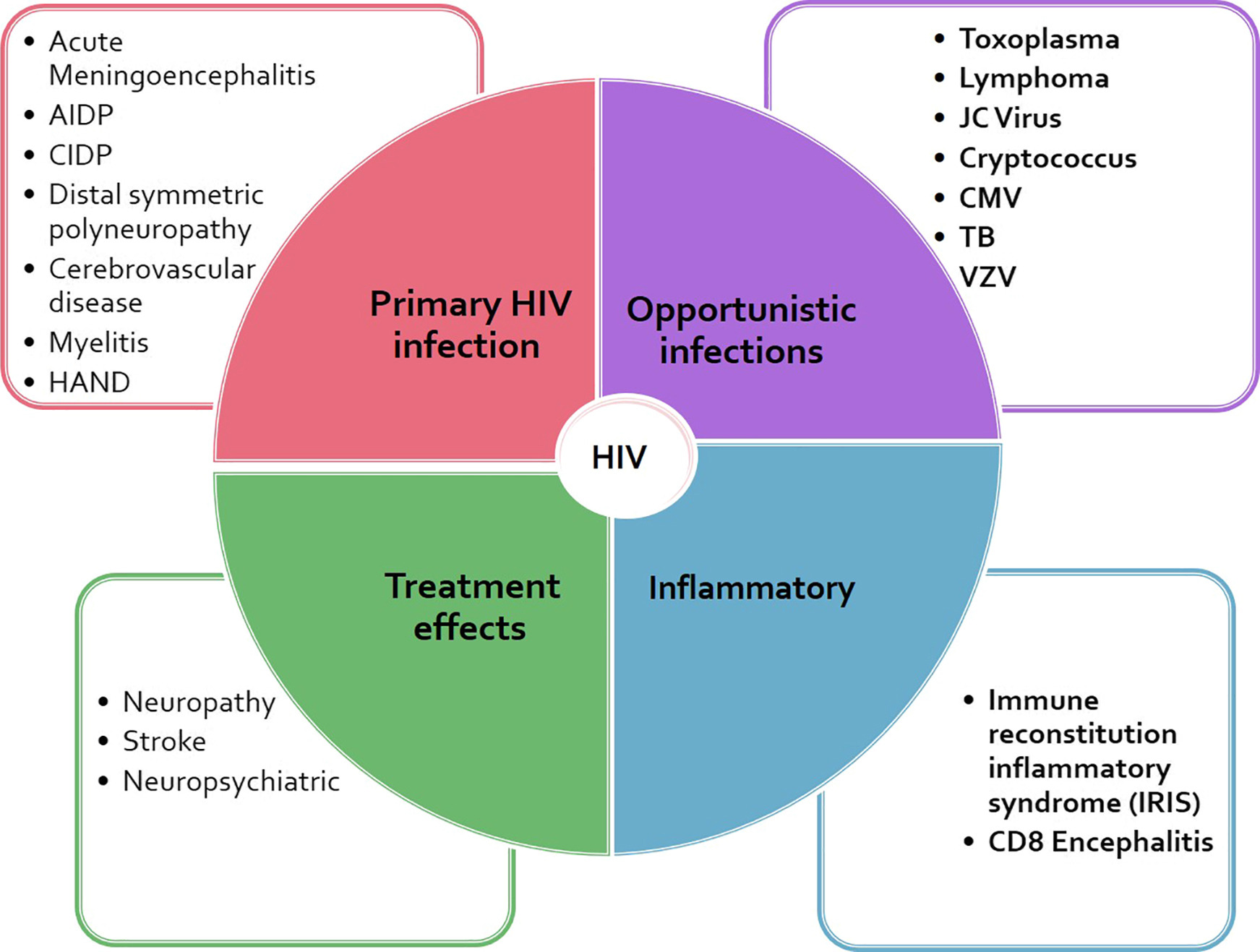
🧠 Neurological disease in advanced HIV/AIDS is common because profound CD4+ T-cell depletion disrupts cell-mediated immunity, allowing (1) opportunistic pathogens (e.g., Toxoplasma, Cryptococcus, JC virus, CMV), (2) HIV-driven neuroinflammation (HAND), and (3) malignancy (primary CNS lymphoma) to emerge. In UK practice, a key “safety rule” is that new focal neurology, seizures, or altered mental status in a person with HIV (or at risk of HIV) should trigger urgent neuroimaging and targeted CSF work-up where safe, in line with NICE’s approach to recognising symptoms needing urgent neurological assessment/referral.
🧪 Immediate approach (UK bedside logic)
- First priorities: ABCDE, check capillary glucose, treat seizures, manage raised ICP.
- Risk stratify by CD4 / ART status:
- CD4 <100: toxoplasmosis, cryptococcus, PML, CMV (and TB/fungal disease depending on exposure).
- CD4 <50: CMV and PCNSL become more likely; multiple OIs may co-exist.
- Imaging before LP if focal deficit, seizures, papilloedema, or reduced GCS (to reduce herniation risk).
- Always think HIV testing in undiagnosed patients with compatible presentations; NICE promotes increasing opportunities to test in appropriate settings.
🧠 HIV-Associated Neurocognitive Disorders (HAND)
- Pathophysiology: persistent CNS viral reservoirs + chronic immune activation → synaptic dysfunction and subcortical “slowing” even with systemic viral suppression in some patients.
- Asymptomatic Neurocognitive Impairment (ANI)
- Objective impairment on neuropsychological testing but no clear functional impact.
- Mild Neurocognitive Disorder (MND)
- Cognitive impairment with measurable impact on day-to-day tasks (attention, executive function, processing speed).
- HIV-Associated Dementia (HAD)
- Severe functional impairment (often motor + behavioural features); now less common with effective ART but still seen in late presenters.
- Management (UK principles): optimise ART, address comorbid drivers (depression, sleep, alcohol/drugs, vascular risk), screen for reversible causes, and avoid unnecessary anticholinergic/sedative burden. (NICE CKS summarises complications that persist despite modern ART.)
🧬 Primary CNS Lymphoma (PCNSL) in AIDS
- About:
- Usually an EBV-associated diffuse large B-cell lymphoma arising in severe immunosuppression.
- Classically occurs with very low CD4 (often <50 cells/µL).
- Clinical clues:
- Headache, seizures, focal deficits, neuropsychiatric change; may mimic toxoplasmosis.
- Diagnosis:
- MRI brain preferred; lesions may enhance and can be solitary or multiple.
- CSF: may show EBV DNA (supportive, not definitive).
- Definitive: stereotactic biopsy where safe/appropriate.
- Important practical point: if biopsy is likely, avoid empiric corticosteroids unless needed for life-threatening mass effect (they can reduce diagnostic yield).
- Treatment (specialist MDT):
- ART + high-dose methotrexate–based regimens are central; radiotherapy may be used in selected cases.
- Management is covered in BHIVA malignancy guidance.
🦠 Opportunistic CNS infections
- Toxoplasma encephalitis
- Mechanism: reactivation of latent Toxoplasma gondii cysts when cellular immunity collapses.
- Exposure: undercooked meat; cat faeces (oocysts).
- Features: headache, fever, confusion, seizures, focal deficits.
- Imaging: typically multiple ring-enhancing lesions with oedema; often basal ganglia/thalamus involvement.
- Testing: serum IgG often positive (prior exposure supports reactivation; a negative IgG makes toxo less likely).
- Treatment: pyrimethamine + sulfadiazine + folinic acid (or alternatives such as pyrimethamine + clindamycin if sulfa-intolerant); then maintenance/secondary prophylaxis until immune reconstitution.
- Cryptococcal meningitis
- Mechanism: inhaled yeast (often C. neoformans) disseminates haematogenously to CNS; high organism burden + raised ICP are major causes of death.
- Features: headache, fever, meningism may be subtle; cranial neuropathies/visual symptoms suggest raised ICP.
- Diagnosis: CSF cryptococcal antigen (high sensitivity) ± India ink; measure opening pressure and manage aggressively if raised.
- Treatment: induction with liposomal amphotericin + flucytosine (then consolidation/maintenance with fluconazole). Modern evidence includes regimens evaluated in large trials such as AMBITION; UK summaries incorporate these data.
- ART timing is critical: unlike many OIs, starting ART too early increases mortality (CNS-IRIS/raised ICP). Guidance commonly recommends deferring ART ~4–6 weeks after starting effective antifungal therapy.
- Progressive Multifocal Leukoencephalopathy (PML)
- Mechanism: JC virus reactivation → oligodendrocyte injury → demyelination.
- Features: progressive focal deficits (weakness, ataxia, visual field loss, dysphasia) with minimal systemic upset.
- MRI: non-enhancing white matter lesions, typically no mass effect/oedema (unless IRIS develops).
- Treatment: immune reconstitution with ART is the main therapy; paradoxical worsening can occur via PML-IRIS, where corticosteroids may be used case-by-case in specialist care.
- CMV encephalitis / ventriculo-encephalitis
- Mechanism: CMV reactivation in profound immunosuppression.
- Features: delirium/encephalopathy, seizures, focal signs; can co-exist with retinitis.
- Treatment: ganciclovir (or valganciclovir) guided by specialist virology/infectious diseases.
🦶 Peripheral neuropathies in HIV
- Distal symmetric polyneuropathy (DSPN)
- Mechanism: HIV neurotoxicity + immune activation; historically also medication-associated with older ART.
- Features: burning pain, paraesthesia, numbness (stocking-glove), reduced ankle jerks.
- Management: optimise ART, exclude/ treat contributors (B12 deficiency, diabetes, alcohol), neuropathic pain approach (often follows general neuropathic pain principles).
- Inflammatory demyelinating polyneuropathy (AIDP/CIDP-like)
- Immune-mediated; may resemble Guillain–Barré.
- Treat with IVIg or plasma exchange in the right clinical context + ART optimisation.
🧍♂️ Myelopathy
- HIV-associated vacuolar myelopathy
- Mechanism: chronic HIV-related spinal cord injury (vacuolation, especially dorsal/lateral columns), often with advanced disease.
- Features: spastic paraparesis, gait disturbance, sensory symptoms, bladder dysfunction.
- Management: ART + rehab; exclude compressive, B12/copper deficiency, and infective causes.
🛡️ Prevention & longer-term management (UK-focused)
- Start and sustain ART: BHIVA advises offering ART to all, typically within 2–4 weeks of diagnosis, with exception pathways for specific CNS OIs (notably cryptococcal meningitis).
- Prophylaxis:
- Use OI prophylaxis in advanced disease and stop/restart based on immune recovery; BHIVA provides CD4/viral-load thresholds (e.g., for PCP prophylaxis discontinuation after sustained CD4 recovery/viral suppression).
- Monitor for CNS-IRIS after ART initiation: paradoxical inflammatory deterioration can occur as immunity returns, especially with high organism burden infections; recognise early because management (including cautious steroids in selected scenarios) can be life-saving.
- NICE referral mindset: persistent abnormal neurological signs/symptoms should trigger timely specialist assessment and investigation pathways rather than watchful waiting when serious secondary causes are plausible.
📚 References (key guidance)
- NICE NG60 HIV testing: increasing uptake (2025).
- NICE NG127 Suspected neurological conditions: recognition and referral (last reviewed 2023).
- NICE CKS HIV infection and AIDS (complications and UK primary care summary).
- BHIVA Opportunistic infections, viral hepatitis and virology (PDF, 2025).
- BHIVA ART guidelines for adults living with HIV-1 (2022).
- BHIVA Malignancy guidelines (PCNSL section) (2014).
- EACS Guidelines v12.0 (2023) (European consensus reference).
- NIH OI guidelines Cryptococcosis: defer ART 4–6 weeks after antifungals (updated 2024).
