
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Reversible cerebral vasoconstriction syndrome (RCVS) ✅
Related Subjects: |Acute Stroke Assessment (ROSIER/NIHSS) |Atrial Fibrillation |Atrial Myxoma |Causes of Stroke |Ischaemic Stroke |Cancer and Stroke |Cardioembolic stroke |CT Basics for Stroke |Endocarditis and Stroke |Haemorrhagic Stroke |Stroke Thrombolysis |Hyperacute Stroke Care |Hypertension |Thrombophilia testing |Cerebral Venous Sinus thrombosis |Small Vessel Disease |CADASIL |CARASIL
🧠 Introduction
- ⚡ Reversible cerebral vasoconstriction syndrome (RCVS) is an important and probably under-recognised cause of thunderclap headache, often mimicking aneurysmal subarachnoid haemorrhage (SAH).
- 👩 It is more common in women, usually presenting in mid-adult life, but it can occur in men and at older ages too.
- 🚨 Although many patients recover well, RCVS can cause convexity SAH, intracerebral haemorrhage, ischaemic stroke, seizures, and posterior reversible encephalopathy syndrome (PRES).
- 📈 Most patients recover well functionally, but the early phase is the dangerous period because this is when haemorrhhagic and ischaemic complications tend to occur.
- 📚 Older names include Call–Fleming syndrome and postpartum angiopathy, but RCVS is the preferred modern umbrella term.
🧬 Pathophysiology
- 🫀 The exact mechanism is not fully understood, but the leading concept is a transient disorder of cerebral arterial tone regulation with abnormal sympathetic overactivity and endothelial dysfunction.
- 🌫️ There is recognised overlap with PRES, suggesting shared disturbances of vascular autoregulation and blood-brain barrier function.
- 🚫 RCVS is not primarily an inflammatory vasculitis, which helps explain why cerebrospinal fluid is often normal or near-normal and why glucocorticoids are generally avoided unless another diagnosis is present.
⚠️ Possible Triggers of RCVS
- ❓ Many cases are associated with a recognisable precipitant, though some remain idiopathic.
- 🤱 Recognised precipitants include the postpartum period and exposure to vasoactive substances.
- 🏃 Thunderclap headaches may be triggered by sex, exertion, Valsalva-type activities such as coughing, sneezing, urinating, or defaecation, and sometimes bathing/showering or sudden head movement.
- 💊 Drug triggers include cannabis, cocaine, amphetamines, serotonergic agents such as SSRIs/SNRIs, triptans, ergot derivatives, and sympathomimetics such as some nasal decongestants.
- 🍷 Other associations include binge alcohol use, phaeochromocytoma, migraine, and occasionally neurosurgical or interventional procedures.
- 🩻 Cervical artery dissection can coexist with RCVS, so it should be actively looked for rather than assumed to be only an alternative diagnosis.
🤱 RCVS was first recognised in reports of postpartum women with transient neurological symptoms and reversible arterial narrowing. That historical entity became known as postpartum angiopathy, but it is now understood as part of the wider RCVS spectrum.
🩺 Clinical Features
- 💥 The hallmark is a thunderclap headache: sudden, very severe headache reaching maximum intensity within 1 minute.
- 🔁 Headaches are often recurrent, occurring over days to weeks, sometimes almost daily early on.
- 🤢 The pain may be diffuse or bilateral, often with nausea, vomiting, photophobia, or a lingering background headache after the initial peak settles.
- 🚨 Some patients develop focal neurological deficits, seizures, visual symptoms, confusion, or encephalopathy because of stroke, haemorrhage, or PRES.
- 👩⚕️ Typical patients are middle-aged women, but absence of this demographic pattern does not exclude the diagnosis.
| 📋 Diagnostic features of RCVS |
|---|
| ⚡ Acute severe headache, usually thunderclap, with or without focal deficits or seizures |
| 🕒 Monophasic course: no new symptoms beyond about 1 month after onset |
| 🩻 Multifocal segmental vasoconstriction of cerebral arteries on CTA, MRA, or catheter angiography |
| 🚫 Exclusion of aneurysmal SAH and other major mimics |
| 🧪 CSF normal or near-normal (important in distinguishing from CNS vasculitis or infection) |
| 🔄 Complete or marked reversal of vasoconstriction, usually by about 12 weeks |
🧠 Differentials of Thunderclap Headache and Stroke
- 🩸 Aneurysmal subarachnoid haemorrhage
- 🔥 Primary angiitis of the CNS (PACNS)
- 🫀 Cervical artery dissection
- 🧫 Cerebral venous sinus thrombosis
- 🌫️ PRES
- 🌀 Migraine or primary thunderclap headache
- 🧠 Pituitary apoplexy
- 🩸 Intracerebral haemorrhage
🔎 Investigations
- 📷 Urgent non-contrast CT head: may be normal, but can show convexity subarachnoid blood, intracerebral haemorrhage, or other complications. Convexity SAH can be very subtle and easy to miss.
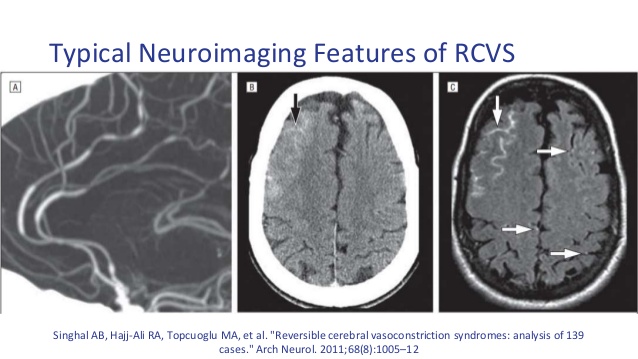
- 🩻 CTA or MRA: may show multifocal arterial narrowing, often described as a “string of beads”. However, vascular imaging can be normal early, and vasoconstriction may peak days later, so repeat imaging is often needed if suspicion remains high.
- 💉 Lumbar puncture: useful when SAH, meningitis, or inflammatory disease needs exclusion and CT is non-diagnostic; CSF in RCVS is usually normal or near-normal.
- 🧲 MRI brain with blood-sensitive sequences and vascular imaging: may show ischaemic infarction, cSAH, ICH, or PRES-type FLAIR hyperintensity. Add MRV if venous thrombosis is a concern and neck vessel imaging if dissection is possible.
- 🛠️ Catheter angiography (DSA): the most sensitive vascular test but invasive; usually reserved for diagnostically difficult cases or where endovascular decisions are needed.
- 📈 Transcranial Doppler: can be used to follow vasoconstriction over time by monitoring flow velocities.
- 🧪 Baseline blood tests should look for mimics and contributors, but inflammatory markers and CSF are typically much less abnormal than in PACNS or infection.
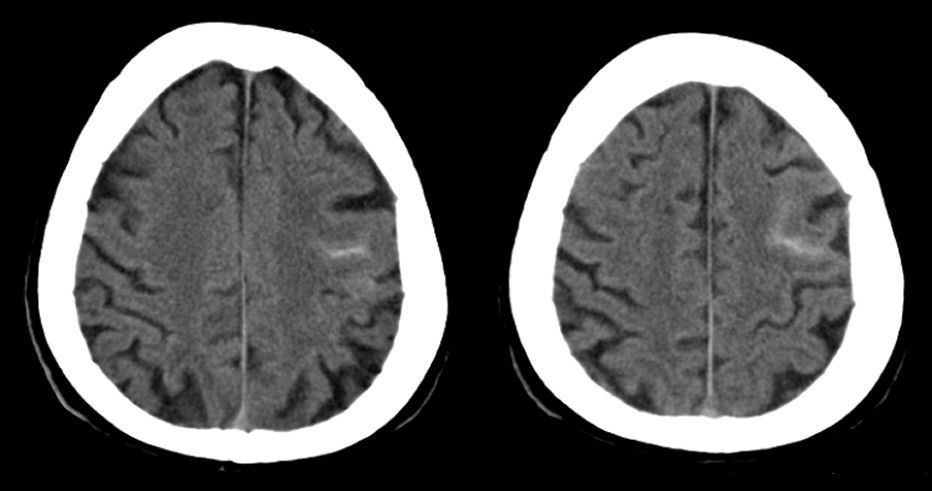
⚠️ Subtle convexity SAH can be very easy to miss. In real-world stroke work this matters because patients with RCVS may present with headache, focal deficit, or seizure and can be mistaken for an ischaemic stroke or migraine. 👀 Careful scrutiny of the cortical sulci and the clinical story is essential. 🔁 Imaging review and repeat vascular imaging are often safer than premature diagnostic closure.
💊 Management
- 🆘 Initial priorities: ABC assessment, pain control, hydration, blood pressure management, and urgent exclusion of aneurysmal SAH and other emergency causes of thunderclap headache.
- 🚫 Remove triggers: stop vasoactive or sympathomimetic drugs where possible, and avoid implicated substances such as cocaine, cannabis, triptans, ergot preparations, and decongestants.
- 💊 Calcium-channel blockers such as nimodipine or verapamil are commonly used for headache relief, but evidence that they prevent stroke or haemorrhagic complications is limited.
- 🧠 Treat complications: seizures, PRES, infarction, haemorrhage, and severe hypertension should be managed according to standard neurovascular practice.
- ⛔ Avoid glucocorticoids unless there is another clear indication, because steroids can worsen outcome in RCVS and are more relevant to CNS vasculitis than to RCVS.
- 🔄 Repeat vascular imaging is important to confirm that the arterial narrowing reverses, usually within about 12 weeks.
📈 Prognosis
- ✅ Most patients recover well, especially if the syndrome is recognised early and triggers are removed.
- ⚠️ However, the early phase is the dangerous period because this is when haemorrhage, PRES, seizures, and ischaemic stroke tend to occur.
- 🔁 Reversibility of the vasoconstriction is a defining feature, typically documented within about 3 months.
📚 References and further reading
- 📖 Singhal AB. Headache Attributed to Reversible Cerebral Vasoconstriction Syndrome and Persistent or Chronic Post-RCVS Headache. 2023.
- 📖 Calabrese LH et al. Narrative Review: Reversible Cerebral Vasoconstriction Syndromes. Ann Intern Med. 2007.
- 📖 Ducros A. Reversible cerebral vasoconstriction syndrome. Lancet Neurol. 2012.
- 📰 BMJ. Assessment and investigation of thunderclap headache. 2025.
- 🏥 Walton Centre NHS Foundation Trust. Reversible cerebral vasoconstriction syndrome (RCVS) patient information leaflet.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery