
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Juvenile Myoclonic epilepsy (JME)
Related Subjects: |Status Epilepticus (Epilepsy) |Coma management |Lorazepam |Phenytoin |Levetiracetam |Epilepsy - General Management |First Seizure |Epilepsy in Pregnancy |Febrile seizures
🧠 About
- Juvenile Myoclonic Epilepsy (JME) is a classic genetic generalised epilepsy. Myoclonic jerks are often misinterpreted as clumsiness, leading to delayed diagnosis.
- ⚠️ Can deteriorate with inappropriate antiseizure medicines (carbamazepine, phenytoin, vigabatrin).
- Non-progressive condition with preserved intellect and normal neurological examination.
🧬 Aetiology & Genetics
- Strong heritable component with altered thalamocortical excitability.
- Positive family history in ~50% of patients.
- Mild female predominance; multiple susceptibility genes suspected rather than a single defect.
📊 Epidemiology
- Prevalence: ~1 in 2000.
- Onset typically between 10–18 years.
- Typical sequence: childhood absence → adolescent myoclonus → generalised tonic–clonic seizures in late teens.
⚡ Seizure Types
- Absence Seizures: Brief lapses in awareness, often shortly after waking.
- Myoclonic Jerks: Sudden bilateral upper-limb jerks within an hour of waking - the classic “🍳 breakfast-time” phenomenon.
- Generalised Tonic–Clonic Seizures: Commonly follow clusters of morning myoclonus.
🔍 Clinical Features & Triggers
- Morning predominance of all seizure types.
- Triggers include sleep loss, alcohol (especially next morning), stress, and photic activation in some.
- No cognitive decline, behavioural regression, or motor deterioration.
🧪 Investigations
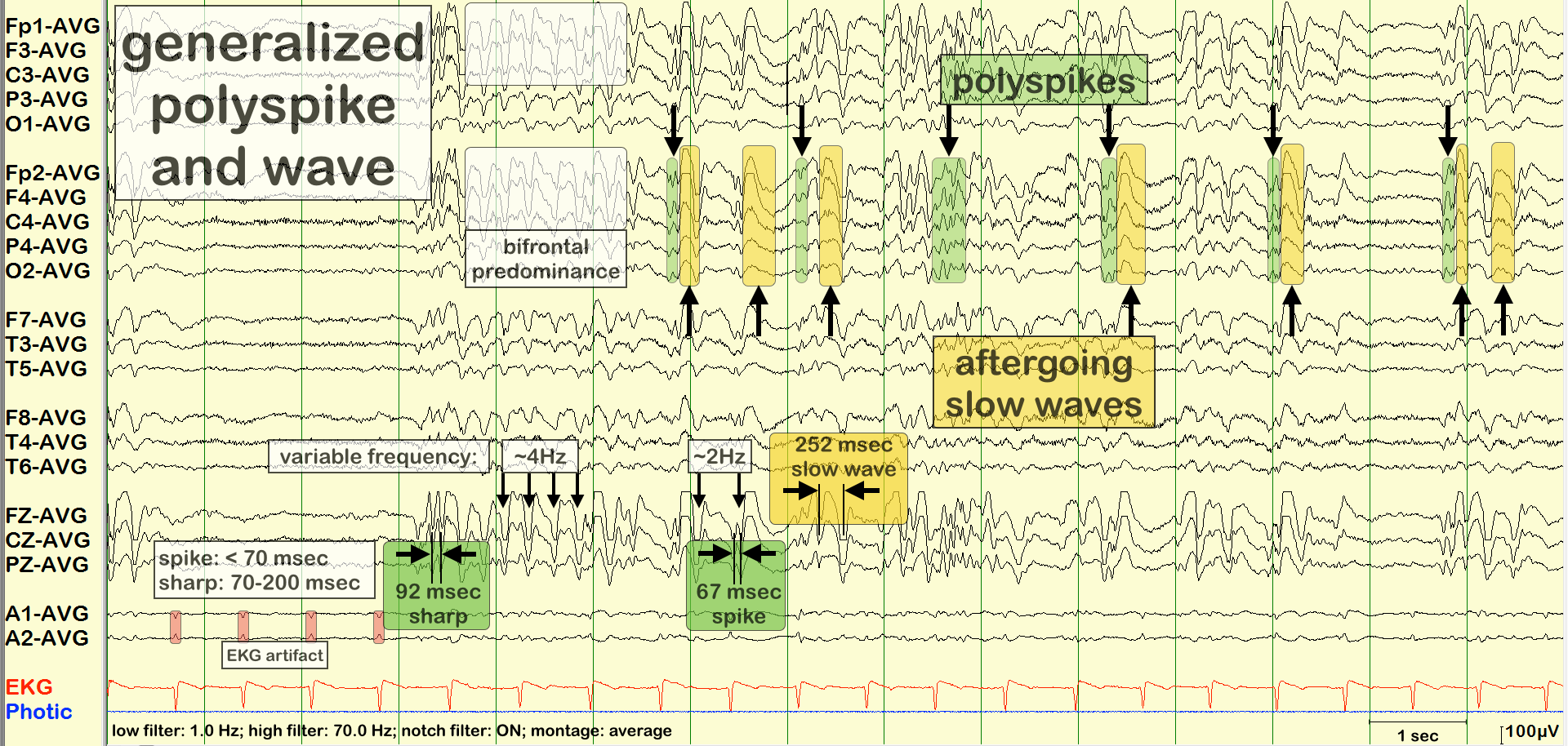
- EEG: Generalised 3–6 Hz polyspike–wave discharges. Markedly enhanced by sleep-deprivation, hyperventilation, or photic stimulation.
- MRI: Typically normal; used to exclude structural mimics.
- Bloods: Normal; performed to rule out metabolic provocation.
💊 Management
- Long-term antiseizure therapy is usually required due to high relapse risk.
- First-line: Sodium valproate (most effective; avoid in women of childbearing potential).
- Alternatives: Levetiracetam, topiramate, lamotrigine (may aggravate myoclonus), and zonisamide.
- Avoid: Carbamazepine, phenytoin, gabapentin, vigabatrin - all may worsen generalised epilepsies.
- Lifestyle: Emphasise sleep hygiene, alcohol moderation, and strict adherence to medication.
📌 References
- Strong heritable component with altered thalamocortical excitability.
- Positive family history in ~50% of patients.
- Mild female predominance; multiple susceptibility genes suspected rather than a single defect.
📊 Epidemiology
- Prevalence: ~1 in 2000.
- Onset typically between 10–18 years.
- Typical sequence: childhood absence → adolescent myoclonus → generalised tonic–clonic seizures in late teens.
⚡ Seizure Types
- Absence Seizures: Brief lapses in awareness, often shortly after waking.
- Myoclonic Jerks: Sudden bilateral upper-limb jerks within an hour of waking - the classic “🍳 breakfast-time” phenomenon.
- Generalised Tonic–Clonic Seizures: Commonly follow clusters of morning myoclonus.
🔍 Clinical Features & Triggers
- Morning predominance of all seizure types.
- Triggers include sleep loss, alcohol (especially next morning), stress, and photic activation in some.
- No cognitive decline, behavioural regression, or motor deterioration.
🧪 Investigations
- EEG: Generalised 3–6 Hz polyspike–wave discharges. Markedly enhanced by sleep-deprivation, hyperventilation, or photic stimulation.
- MRI: Typically normal; used to exclude structural mimics.
- Bloods: Normal; performed to rule out metabolic provocation.
💊 Management
- Long-term antiseizure therapy is usually required due to high relapse risk.
- First-line: Sodium valproate (most effective; avoid in women of childbearing potential).
- Alternatives: Levetiracetam, topiramate, lamotrigine (may aggravate myoclonus), and zonisamide.
- Avoid: Carbamazepine, phenytoin, gabapentin, vigabatrin - all may worsen generalised epilepsies.
- Lifestyle: Emphasise sleep hygiene, alcohol moderation, and strict adherence to medication.
📌 References
- Absence Seizures: Brief lapses in awareness, often shortly after waking.
- Myoclonic Jerks: Sudden bilateral upper-limb jerks within an hour of waking - the classic “🍳 breakfast-time” phenomenon.
- Generalised Tonic–Clonic Seizures: Commonly follow clusters of morning myoclonus.
🔍 Clinical Features & Triggers
- Morning predominance of all seizure types.
- Triggers include sleep loss, alcohol (especially next morning), stress, and photic activation in some.
- No cognitive decline, behavioural regression, or motor deterioration.
🧪 Investigations
- EEG: Generalised 3–6 Hz polyspike–wave discharges. Markedly enhanced by sleep-deprivation, hyperventilation, or photic stimulation.
- MRI: Typically normal; used to exclude structural mimics.
- Bloods: Normal; performed to rule out metabolic provocation.
💊 Management
- Long-term antiseizure therapy is usually required due to high relapse risk.
- First-line: Sodium valproate (most effective; avoid in women of childbearing potential).
- Alternatives: Levetiracetam, topiramate, lamotrigine (may aggravate myoclonus), and zonisamide.
- Avoid: Carbamazepine, phenytoin, gabapentin, vigabatrin - all may worsen generalised epilepsies.
- Lifestyle: Emphasise sleep hygiene, alcohol moderation, and strict adherence to medication.
📌 References
- EEG: Generalised 3–6 Hz polyspike–wave discharges. Markedly enhanced by sleep-deprivation, hyperventilation, or photic stimulation.
- MRI: Typically normal; used to exclude structural mimics.
- Bloods: Normal; performed to rule out metabolic provocation.
💊 Management
- Long-term antiseizure therapy is usually required due to high relapse risk.
- First-line: Sodium valproate (most effective; avoid in women of childbearing potential).
- Alternatives: Levetiracetam, topiramate, lamotrigine (may aggravate myoclonus), and zonisamide.
- Avoid: Carbamazepine, phenytoin, gabapentin, vigabatrin - all may worsen generalised epilepsies.
- Lifestyle: Emphasise sleep hygiene, alcohol moderation, and strict adherence to medication.
📌 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery