
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Corticospinal Tract
🧠 The corticospinal tract is the main descending motor pathway for voluntary movement, especially precise, fractionated movements of the distal limbs such as finger and hand control. It links the motor cortex to spinal motor circuits, so it is one of the most important pathways for neurological localisation. Damage anywhere along this tract produces a recognisable pattern of weakness and, if the lesion is above the anterior horn cell, classic upper motor neuron (UMN) signs.
📖 Overview
The corticospinal tract is part of the wider pyramidal motor system. Its job is not simply to “turn muscles on”, but to provide skilled voluntary control, especially over distal flexors and fine finger movements. Other descending pathways such as the reticulospinal, vestibulospinal, and rubrospinal tracts also influence posture and movement, but the corticospinal tract is the pathway most classically associated with UMN weakness.
📍 Origin – Motor Cortex
Corticospinal fibres arise predominantly from layer V pyramidal neurons in the frontal lobe, including the primary motor cortex of the precentral gyrus. Additional fibres arise from the premotor cortex and supplementary motor area, which help translate motor planning into execution. Some fibres also arise from the primary somatosensory cortex, helping modulate sensory input during movement.
- Primary motor cortex (M1): major source of fast, powerful descending motor output
- Premotor cortex: involved in preparation and externally guided movement
- Supplementary motor area: involved in internally generated and sequenced movement
- Somatotopic organisation: leg more medial, arm/hand superior-lateral, face most lateral
- Betz cells: giant pyramidal neurons that contribute some large fast-conducting fibres
🗺️ Motor Homunculus
The motor cortex is arranged somatotopically as the motor homunculus. Body parts requiring fine motor control, especially the hand, thumb, and face, occupy disproportionately large cortical areas. This explains why cortical lesions often produce especially obvious weakness or clumsiness of the hand and lower face.
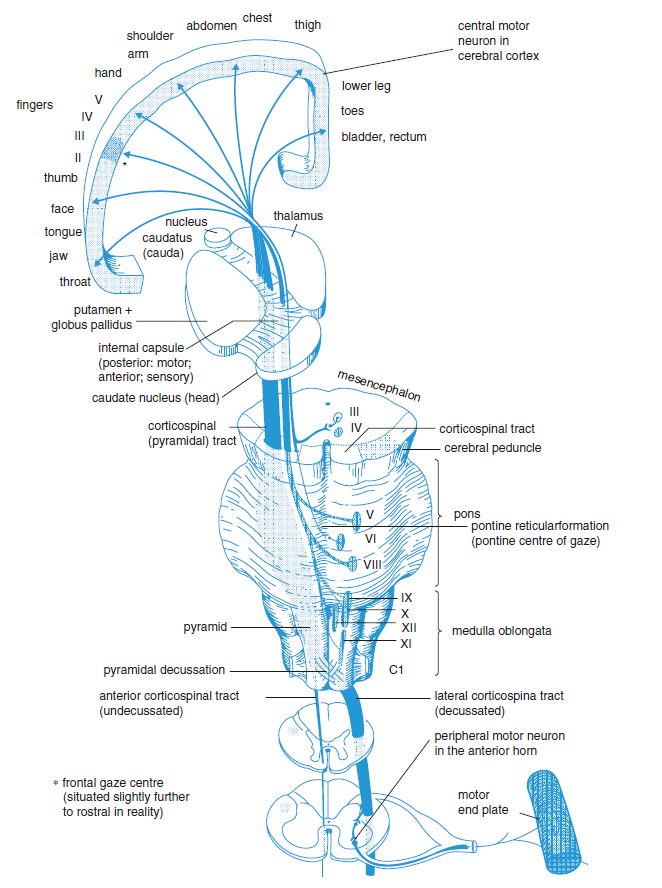
🧭 Course Through the Cerebrum
From the cortex, fibres descend through the corona radiata and then converge into the posterior limb of the internal capsule. This is a major anatomical bottleneck: a relatively small lesion here can interrupt a very large number of tightly packed fibres, causing a dense contralateral hemiparesis. From there, the tract passes into the brainstem.
- Corona radiata – fibres fan out beneath the cortex
- Posterior limb of internal capsule – dense compact bundle; high-yield stroke site
- Genu/internal capsule vicinity – corticobulbar fibres for cranial nerves run nearby
🧠 Course Through the Brainstem
After the internal capsule, corticospinal fibres pass through the crus cerebri of the midbrain, then through the basis pontis, and finally form the medullary pyramids in the ventral medulla. The name “pyramidal tract” comes from these visible medullary pyramids.
- Midbrain: crus cerebri / cerebral peduncles
- Pons: ventral (basis) pons, broken up by pontine nuclei and transverse fibres
- Medulla: ventral pyramids
🔁 Pyramidal Decussation
At the caudal medulla, about 85–90% of corticospinal fibres cross in the pyramidal decussation. These crossed fibres descend in the lateral corticospinal tract, which is the main pathway controlling distal limb muscles. The remaining uncrossed fibres descend as the anterior corticospinal tract, influencing axial and proximal muscles, and many of these eventually cross near their spinal level of termination.
- Decussation: lower medulla
- Lateral corticospinal tract: crossed fibres, mainly distal limb control
- Anterior corticospinal tract: mainly uncrossed initially, more axial/proximal influence
- Key localisation rule: above the decussation = contralateral weakness; below it = ipsilateral weakness
🦴 Course in the Spinal Cord
Within the spinal cord, the lateral corticospinal tract descends in the lateral funiculus. Fibres terminate at different spinal levels depending on the muscles they control. They synapse either directly onto alpha motor neurons or, more commonly, via spinal interneurons. Direct cortico-motoneuronal connections are especially important in the hand, allowing highly fractionated finger movement.
- Lateral funiculus: site of the lateral corticospinal tract
- Anterior horn: final common pathway for movement
- Interneurons: important for patterning and modulation of output
- Direct monosynaptic input: especially relevant to fine distal hand control
⚙️ Function
The corticospinal tract is particularly important for voluntary, skilled, fractionated movement, especially in the distal upper limb. It helps suppress primitive mass movement patterns and allows selective recruitment of individual muscle groups. This is why corticospinal lesions cause not only weakness, but also loss of dexterity and a tendency toward more stereotyped movement patterns.
- ✋ Fine finger and hand movements
- 🎯 Precise voluntary targeting of movement
- 🧩 Fractionation of complex muscle activity
- 🛑 Inhibitory modulation of spinal reflex circuits
⚠️ Upper vs Lower Motor Neuron Lesions
The corticospinal tract defines the concept of the upper motor neuron. A lesion anywhere from the cortex down to just before the anterior horn cell produces a characteristic UMN syndrome. By contrast, lesions affecting the anterior horn cell, peripheral nerve, neuromuscular junction, or muscle produce LMN-pattern weakness.
- UMN signs: weakness, increased tone (spasticity), hyperreflexia, clonus, extensor plantar response
- LMN signs: weakness, wasting, fasciculations, reduced tone, hyporeflexia
- Early UMN lesions may be initially flaccid before spasticity develops
🧪 Why UMN Signs Occur
UMN signs reflect loss of descending inhibitory control over spinal reflex circuits. Without normal cortical modulation, stretch reflexes become exaggerated, tone increases in a velocity-dependent way, and pathological reflexes such as the Babinski response emerge. Weakness is typically more pronounced in extensors of the upper limb and flexors of the lower limb, contributing to the classic spastic hemiparetic posture.
🩺 Clinical Correlation – Localisation Along the Tract
Localising corticospinal lesions becomes much easier if you ask where the lesion is relative to the decussation, and whether there are associated cortical, brainstem, or spinal features. The pattern of weakness and associated signs often tells you the anatomical level.
- Cortex: contralateral weakness, often with cortical signs such as aphasia, neglect, visual field defect, or seizures
- Internal capsule: dense contralateral face-arm-leg weakness with no major cortical sensory or visual features
- Brainstem: “crossed signs” - ipsilateral cranial nerve deficit with contralateral limb weakness
- Spinal cord: ipsilateral UMN weakness below the lesion, often with a sensory level and sphincter disturbance
- Hemicord lesion: ipsilateral corticospinal weakness below the lesion as part of Brown-Séquard syndrome
🧠 Classic High-Yield Examples
- Lacunar infarct of the posterior limb of the internal capsule: pure motor hemiparesis
- Midbrain lesion: contralateral hemiparesis with ipsilateral oculomotor palsy
- Cervical cord compression: bilateral leg weakness progressing to spastic quadriparesis depending on level
- Multiple sclerosis plaque in the cervical cord: UMN weakness with sensory symptoms and possible Lhermitte’s phenomenon
- Motor neuron disease: mixed UMN and LMN signs because both corticospinal pathways and anterior horn cells are affected
🦶 Plantar Response
The extensor plantar response (Babinski sign) is a classic marker of corticospinal tract dysfunction. Stroking the lateral sole leads to dorsiflexion of the great toe, often with fanning of the others. In adults this is abnormal and suggests an UMN lesion; in infants it can be normal because corticospinal pathways are not yet fully myelinated.
🚶 Effect on Gait
Corticospinal lesions often alter gait. A unilateral lesion may produce a spastic hemiparetic gait with circumduction of the leg and flexed posture of the arm. Bilateral tract involvement, especially in the spinal cord, may cause a spastic paraparesis with stiff, scissoring gait and difficulty initiating smooth leg swing.
🔍 Common Causes of Corticospinal Tract Lesions
- 🩸 Stroke – cortical, capsular, brainstem
- 🧠 Brain tumour or metastasis
- 🔥 Multiple sclerosis and other inflammatory demyelinating disease
- 🦴 Cervical spondylotic myelopathy or cord compression
- 🚑 Trauma to brain or spinal cord
- 🧬 Motor neuron disease
- 🦠 Infection or inflammatory myelopathy
🎓 Exam Pearls
- Above the pyramidal decussation = contralateral weakness
- Below the decussation = ipsilateral weakness
- Internal capsule lesions can cause dense weakness because fibres are tightly packed
- Lateral corticospinal tract is the major tract for distal limb control
- UMN lesion = weakness + spasticity + hyperreflexia + extensor plantar
- Brainstem lesion often gives crossed cranial nerve and long tract signs
- Spinal cord lesion often adds a sensory level and bladder symptoms
🧠 Teaching Pearl
Ask two localisation questions every time you see weakness: is it ipsilateral or contralateral to the lesion? and are UMN signs present? Once you know where the corticospinal fibres cross, neurological localisation becomes a matter of anatomy rather than memory. This is one of the most high-yield pathways in bedside neurology because it links pattern recognition, clinical examination, and lesion localisation so neatly.
📝 One-Line Summary
The corticospinal tract is the main voluntary motor pathway from cortex to spinal cord; lesions above the decussation cause contralateral UMN weakness, lesions below it cause ipsilateral UMN weakness, and the associated signs help pinpoint the anatomical level.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery