
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Herpes Simplex Encephalitis (HSV)
Related Subjects: |Herpes Varicella-Zoster (Shingles) Infection |Chickenpox Varicella Infection |Varicella Cerebral Vasculopathy |Herpes Viruses |Herpes Zoster Ophthalmicus (HZO) Shingles |MonkeyPox |Mumps |Measles |Rubella (German Measles) |Epstein-Barr Virus infection |Cytomegalovirus (CMV) infections |CMV retinitis infections |Toxoplasmosis
⚡ Key Clinical Pearl: Always treat suspected HSVE with IV Aciclovir if it’s in the differential. HSVE can mimic a middle cerebral artery (MCA) stroke but clues such as fever 🌡️, seizures ⚡, confusion 🌀, and temporal lobe changes on MRI 🧠 should raise suspicion. It occurs in about 1 per 3,000 stroke cases, meaning a typical UK stroke unit may see one case every 5–10 years.
🧠 About
- HSVE is the most serious form of herpes encephalitis, typically caused by HSV-1 in adults.
- Other viral causes include HSV-2 (more common in neonates) and rarely West Nile virus.
📊 Epidemiology
- Incidence: ~1 case per million per year.
- UK: ~50–100 cases annually, about half in patients >50 years old.
- Presentation can be fulminant with coma, or initially stroke-like ➝ deterioration over hours–days.
- Estimated 12–25 patients per year in the UK present as stroke mimics out of ~100,000 annual strokes.
🦠 Virology & Aetiology
- 90% of adults are seropositive for HSV-1 (latent in trigeminal ganglion).
- Reactivation may occur with stress, trauma, immunosuppression, sunlight ☀️, menstruation, or infection.
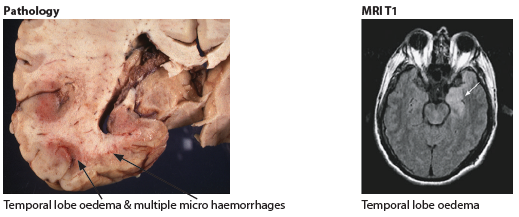
- Predilection for the temporal lobes and limbic system ➝ causes haemorrhagic necrosis 💉.
- Spread can be unilateral ➝ bilateral but asymmetric involvement.
🧬 Pathology
- Haemorrhagic necrosis of the inferomedial temporal lobes.
- Limbic system involvement ➝ psychiatric changes, seizures, memory deficits.
- Histology: Cowdry Type A intranuclear inclusions in infected neurons.
🩺 Clinical Features
- Headache + fever + seizures ⚡
- Cold sores on lips or mouth (recent HSV reactivation) 👄
- Confusion, altered behaviour, personality change
- Speech abnormalities, focal deficits (hemiparesis, hyperreflexia)
- Severe cases: coma, raised ICP, death ☠️
- Can appear identical to a stroke with dysphasia and cognitive issues
🔍 Investigations
- FBC: Raised WCC.
- U&E: Hyponatraemia in ~50% (also seen in ~35% of strokes).
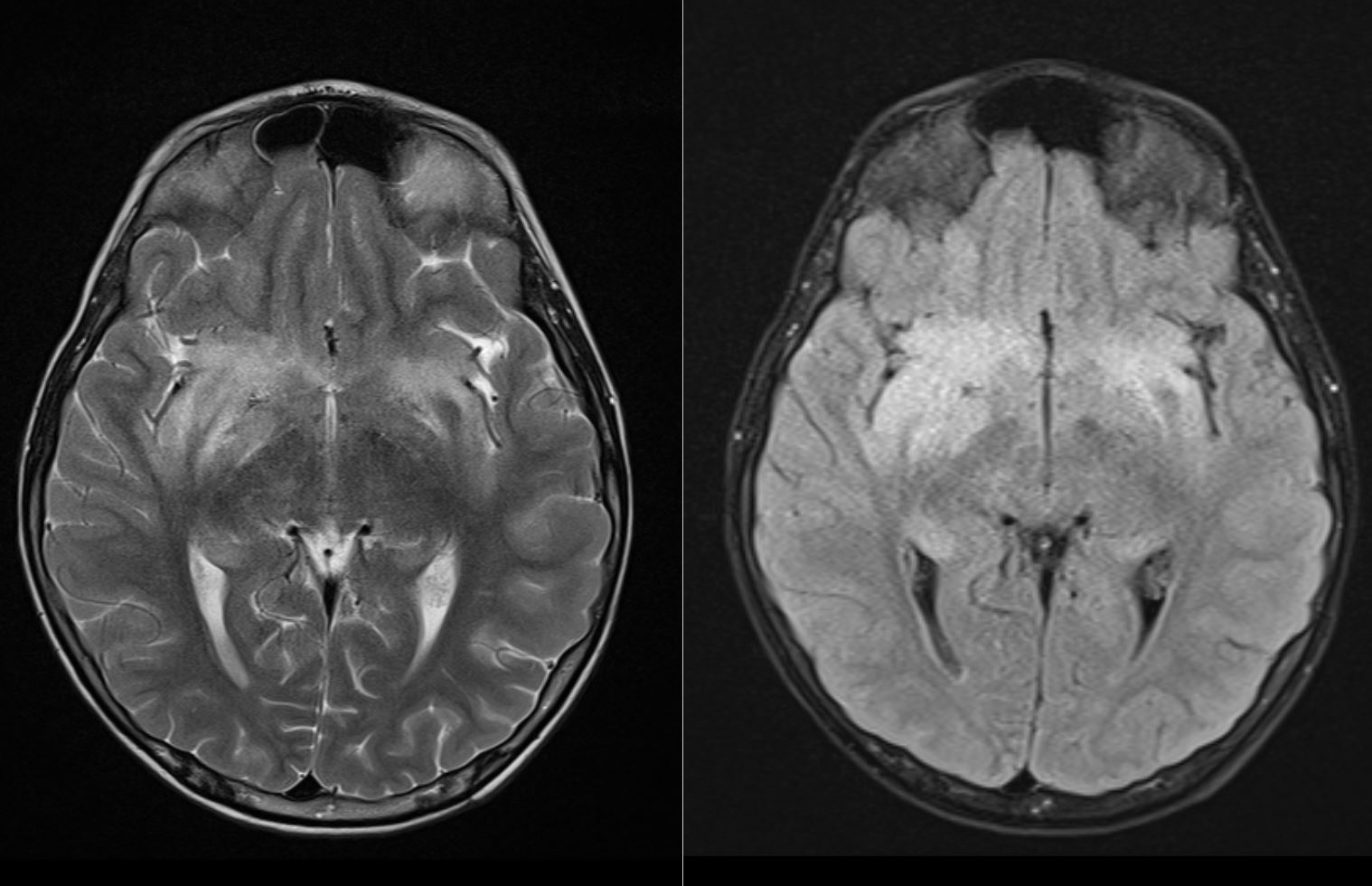
- CT/MRI: Temporal lobe oedema, necrosis, haemorrhage; restricted diffusion less intense than stroke.
- CSF: Lymphocytosis, ↑ protein, sometimes blood-stained. HSV PCR = gold standard.
- EEG: Focal temporal slowing, periodic discharges.
- Brain biopsy: Rare, but may show Cowdry A inclusions.
🖼️ Imaging Examples
 📖 HSVE should always be in the differential for patients with temporal lobe changes, psychiatric symptoms + seizures.
👉 Stroke mimics in otherwise “well” patients should trigger early MRI and CSF PCR testing.
📖 HSVE should always be in the differential for patients with temporal lobe changes, psychiatric symptoms + seizures.
👉 Stroke mimics in otherwise “well” patients should trigger early MRI and CSF PCR testing.
📖 References
Cases - Herpes Simplex Encephalitis (HSV)
- Case 1 - Acute Confusion and Seizure: A 32-year-old woman presents with fever, headache, and a generalised tonic-clonic seizure. She is drowsy and disoriented. MRI brain: hyperintense lesions in the temporal lobe. CSF: lymphocytic pleocytosis, raised protein, normal glucose. Diagnosis: HSV encephalitis (classic temporal lobe involvement). Management: Immediate IV aciclovir; supportive neuro-ICU care; EEG monitoring if recurrent seizures.
- Case 2 - Psychiatric Presentation: A 24-year-old man develops acute personality change, bizarre behaviour, and hallucinations. No prior psychiatric history. He then develops fever and expressive dysphasia. Diagnosis: HSV encephalitis masquerading as acute psychosis. Management: Urgent IV aciclovir before confirmatory LP/PCR; neuro and psych liaison; seizure precautions.
- Case 3 - Elderly Patient with Delayed Diagnosis: A 70-year-old man is admitted with progressive confusion, fever, and focal seizures over 3 days. Initially treated as delirium. CT head normal, but MRI shows temporal lobe oedema with haemorrhagic change. CSF PCR: HSV-1 DNA positive. Diagnosis: HSV-1 encephalitis (delayed recognition). Management: High-dose IV aciclovir for 14–21 days; monitor renal function; rehabilitation for cognitive and speech deficits.
- Case 4 - Stroke Mimic in an Older Adult: A 68-year-old woman is brought to the ED with sudden-onset confusion, expressive aphasia, and right-sided weakness. Paramedics activated a stroke call. CT head shows no acute infarct. She spikes a fever in hospital and has a focal seizure. MRI reveals left temporal lobe oedema with haemorrhagic changes. CSF PCR is positive for HSV-1. Diagnosis: HSV encephalitis presenting as a stroke mimic (left temporal lobe involvement). Management: Immediate IV aciclovir; supportive care in neuro-ICU; speech and rehabilitation therapy post-acute phase.
Teaching Commentary 🧠
HSV encephalitis is the most common cause of sporadic fatal viral encephalitis, classically due to HSV-1 (HSV-2 more in neonates). Hallmarks: - Fever, headache, confusion, seizures. - Predilection for temporal lobes → dysphasia, hallucinations, behavioural changes. - MRI: temporal lobe hyperintensity ± haemorrhage. - CSF: lymphocytes, ↑protein, normal glucose; PCR confirms HSV. Immediate IV aciclovir should be started empirically (delay worsens prognosis). Complications: seizures, long-term cognitive impairment. Mortality untreated ≈70%, but with treatment ≈20%.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery