General Basic Fracture management ✅
Related Subjects:
|Fracture management basics
|Fractured Neck of Femur
|Fractured Shaft Femur
|Fractured Femur Supracondylar Fractures
|Fractured Femur
|Fractured Tibia and Fibula
Fracture Management 🦴 follows the sequence:
👉 ABCDE → Analgesia → Assessment → Imaging → Reduction / Immobilisation → Definitive Management → Rehabilitation.
Always prioritise life before limb in the trauma patient. In UK practice, fracture care should follow the wider trauma framework in NICE major trauma guidance, with fracture-specific decisions guided by NICE NG38 (non-complex fractures), NICE NG37 (complex fractures), and BOAST standards.
📖 About
- A fracture is a break in the continuity of bone, which may be complete or incomplete.
- Fractures may result from acute trauma, repetitive loading, or abnormal bone weakened by disease.
- In practice, fractures range from simple stable injuries managed in a splint to limb-threatening or life-threatening trauma requiring urgent multidisciplinary care.
⚙️ Aetiology
- Direct trauma: force applied directly at the fracture site, for example a tibial shaft fracture after a direct blow.
- Indirect trauma: force transmitted through a limb, for example a fall onto an outstretched hand causing a distal radius, clavicle, or supracondylar injury.
- Twisting injury: commonly causes spiral fractures, especially in long bones.
- Stress fracture: repetitive microtrauma exceeding the bone’s ability to remodel, seen in athletes and military recruits.
- Insufficiency fracture: normal force through weakened bone, often due to osteoporosis, osteomalacia, or other metabolic bone disease.
- Pathological fracture: fracture through bone weakened by tumour, infection, cyst, Paget disease, or other structural pathology.
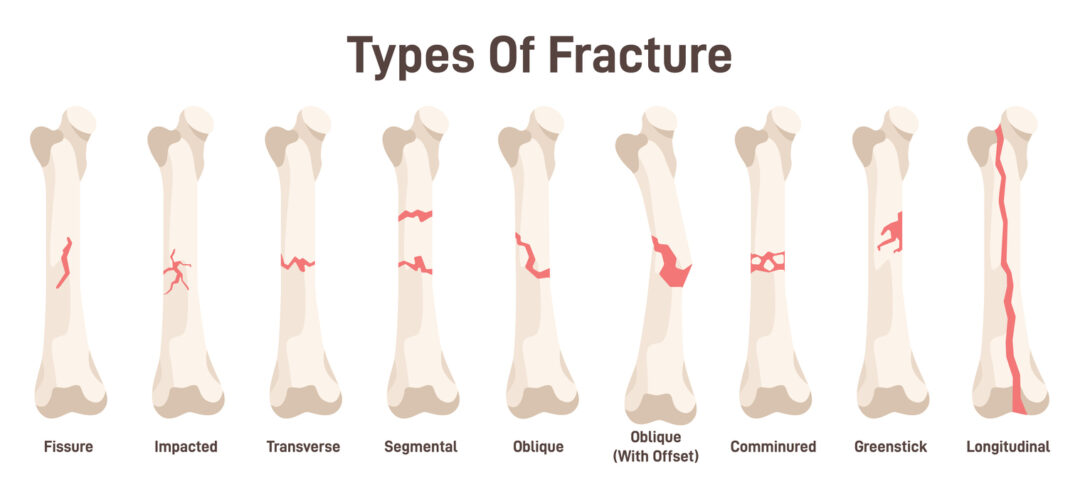
🔎 Types of Fracture
- By skin integrity: open (skin breach communicates with fracture or deep tissues) 🚨 vs closed.
- By displacement: undisplaced, angulated, translated, shortened, rotated, impacted.
- By completeness: complete vs incomplete.
- By pattern: transverse, oblique, spiral, comminuted, segmental.
- By relation to joint: intra-articular vs extra-articular.
- By mechanism: avulsion, stress, crush, burst, compression.
- Paediatric patterns: greenstick, buckle (torus), physeal / Salter-Harris injuries 👶.
- Fracture-dislocation: fracture associated with joint dislocation.
🩺 Initial Clinical Assessment
- Start with ABCDE, especially in high-energy trauma or when multiple injuries are possible.
- History: mechanism of injury, time since injury, open wound, contamination, inability to weight-bear or use the limb, comorbidities, anticoagulants, steroids, bisphosphonates, osteoporosis risk, tetanus status, and baseline function.
- Mechanism matters: low-energy fragility injuries and high-energy trauma raise very different diagnostic and management priorities.
- Examine the whole limb, and always assess the joint above and below.
- Document neurovascular status carefully: pulses, capillary refill, temperature, colour, motor function, and sensory function.
- Repeat neurovascular examination after splinting, reduction, or any deterioration. This is explicitly emphasised in BOAST open fracture standards.
👀 LOOK, FEEL, MOVE, ADDITIONAL
- LOOK: deformity, swelling, bruising, open wounds, skin tenting, shortening, rotation, and distal perfusion.
- FEEL: bony tenderness, crepitus, compartment tension, distal pulses, and sensory deficit.
- MOVE: active and passive movement where safe, and function of joints above and below.
- ADDITIONAL: hand dominance for upper limb injuries, weight-bearing status for lower limb injuries, occupation, mobility aids, and baseline frailty.
🚨 Red Flags Not to Miss
- Open fracture – any wound near a fracture should be assumed open until proven otherwise.
- Compartment syndrome – classically pain out of proportion and pain on passive stretch are early features; paraesthesia is concerning; pallor, pulselessness, and paralysis are late signs.
- Neurovascular compromise – absent pulses, ischaemia, dense sensory loss, or evolving motor deficit.
- Skin threat / tenting – risk of conversion to an open fracture.
- Associated dislocation – especially knee, ankle, hip, elbow, and perilunate injuries.
- High-energy mechanism – suspect associated head, chest, abdominal, pelvic, and spinal injuries.
- Non-accidental injury – particularly in children, frail adults, or where the history does not fit the injury.
🧪 Investigations
- X-ray: first-line for most fractures. Obtain at least two orthogonal views. Include the whole bone and adjacent joints when clinically relevant.
- CT: useful for complex intra-articular fractures, pelvis, spine, occult extension, pre-operative planning, and high-energy injuries. NICE recommends CT first-line in adults with suspected high-energy pelvic fractures.
- MRI: preferred for occult fractures, stress fractures, scaphoid injury, marrow oedema, and associated soft-tissue injury. NICE recommends considering MRI as first-line imaging for suspected scaphoid fracture after clinical examination.
- Ultrasound: occasionally helpful in selected paediatric injuries or soft-tissue assessment, but not a routine replacement for X-ray.
- Blood tests: FBC, U&Es, clotting, group and save / crossmatch as indicated, especially in femoral, pelvic, open, or polytrauma injuries.
- Trauma CT: in major trauma, imaging strategy should be integrated into the overall trauma pathway rather than ordered as isolated limb imaging. BOAST notes that trauma CT protocols should maximise useful information while minimising delay.
📸 Imaging Rules and NICE Guidance
- Suspected knee fracture: use the Ottawa knee rules in people over 2 years to determine the need for X-ray.
- Suspected ankle / foot fracture: use the Ottawa ankle and foot rules in people over 5 years.
- ED fracture X-rays: NICE states that the definitive written report should be available before discharge from the emergency department.
- High-energy pelvic trauma: use CT first-line in adults. If active bleeding is suspected after blunt high-energy trauma, apply a purpose-made pelvic binder.
💊 Analgesia
- Give analgesia early and reassess regularly.
- Use a multimodal approach: paracetamol, NSAIDs if appropriate, opioids when needed, and regional anaesthesia where indicated.
- NICE specifically recommends considering a femoral nerve block or fascia iliaca block in children under 16 with suspected displaced femoral fractures.
- For dorsally displaced distal radius fractures in adults, NICE recommends considering intravenous regional anaesthesia (Bier’s block) if reduction is performed in the emergency department, and advises not to use nitrous oxide/oxygen alone for reduction.
🛠️ Core Principles of Management
- Reduction: restore alignment, length, and rotation where required.
- Immobilisation / Stabilisation: splint, sling, cast, backslab, traction, external fixation, or internal fixation depending on the fracture pattern and soft-tissue injury.
- Definitive management: conservative or operative, depending on stability, displacement, joint involvement, open injury, soft-tissue status, and patient factors.
- Rehabilitation: early safe mobilisation, physiotherapy, occupational therapy, falls assessment, and bone health review where relevant.
🔧 Reduction
- Closed reduction: manipulation under analgesia, sedation, haematoma block, regional block, or anaesthesia.
- Open reduction: surgical exposure to restore anatomy, usually combined with internal fixation when closed methods are inadequate.
- After any reduction: repeat and document the neurovascular examination, obtain check imaging, and reassess pain and compartment status.
🩹 Immobilisation and Splintage
- Splint early to reduce pain, bleeding, and soft-tissue damage.
- BOAST open fracture standards state that the limb should be realigned and splinted.{index=11}
- In pre-hospital care, NICE recommends considering a traction splint or adjacent leg as a splint for suspected long-bone fractures above the knee, and a vacuum splint for other long-bone leg fractures.
- Avoid circumferential casts in very swollen fresh injuries when a backslab or splint is safer.
🚨 Open Fractures – NICE and BOAST Principles
- Assume any fracture with an overlying wound is open until proven otherwise.
- Do not repeatedly explore or irrigate the wound in ED. NICE specifically advises not to irrigate open fractures of the long bones, hindfoot, or midfoot in the emergency department before formal wound excision.
- Apply a saline-soaked dressing covered with an occlusive layer.
- Give IV antibiotics immediately if not already given. NICE recommends prophylactic IV antibiotics as soon as possible, ideally within 1 hour of injury in the pre-hospital setting when feasible, and immediately in ED if not yet given.
- Check tetanus status and manage according to local policy.
- Immobilise the limb and obtain urgent orthopaedic input.
- For open fractures of long bone, hindfoot, or midfoot, NICE recommends management through a combined orthoplastic approach.
- NICE timing:
- Immediate wound excision for highly contaminated open fractures
- Within 12 hours for high-energy open fractures likely to be Gustilo IIIA or IIIB that are not highly contaminated
- Within 24 hours for all other open fractures
- Definitive fixation and soft-tissue cover should be coordinated with orthoplastics; if internal fixation is used, definitive soft-tissue cover should occur at the same time.
🏥 Surgical Indications (General)
- Open fracture
- Neurovascular compromise
- Compartment syndrome
- Fracture-dislocation or irreducible dislocation
- Unstable displaced fracture
- Intra-articular displacement / incongruity
- Failure of closed reduction or inability to maintain alignment
- Polytrauma where operative stabilisation improves overall care
- Pathological fracture requiring biopsy and fixation planning
🧒 Important NICE Fracture-Specific Points
- Distal radius torus fractures in children: NICE says do not use a rigid cast, and children can usually be discharged after first assessment without routine follow-up.
- Unimalleolar ankle fractures managed non-operatively: advise immediate unrestricted weight-bearing as tolerated, with follow-up within 2 weeks if stability is uncertain.
- Ankle fractures requiring surgery: NICE advises considering surgery on the day of injury or the next day.
- Hip fractures in adults: these follow a separate NICE pathway with emphasis on early surgery and coordinated multidisciplinary care.
📦 Rehabilitation and Secondary Prevention
- Encourage early safe mobilisation once the fracture is stabilised and it is clinically appropriate.
- Involve physiotherapy and occupational therapy early for gait, transfers, upper-limb function, and discharge planning.
- For fragility fractures, assess for osteoporosis, falls risk, vitamin D issues, and future fracture prevention.
- Document weight-bearing status clearly: non-weight-bearing, touch, partial, or full weight-bearing as tolerated.
📌 OSCE / Exam Pearls
- Always document neurovascular status before and after manipulation or splinting.
- Pain out of proportion and pain on passive stretch are early clues to compartment syndrome.
- Any wound near a fracture = open fracture until proven otherwise.
- Do not irrigate open long-bone, hindfoot, or midfoot fractures in ED before formal wound excision.
- Ottawa rules are examinable and useful.
- For suspected scaphoid fracture, modern NICE guidance favours early MRI rather than repeated delayed plain films.
📚 References
