
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Carotid Endarterectomy ✅
Related Subjects: Renal Colic | Abdominal Aortic Aneurysm | Acute Abdominal Pain | Assessing Abdominal Pain | Penetrating Abdominal Trauma | Peripheral Arterial Disease (PAD) |Abdominal Aortic Aneurysm (AAA) | Carotid Endarterectomy | Buerger's disease (Thromboangiitis obliterans ) | Leriche syndrome (aortoiliac occlusive disease) | Vascular Surgery: Introduction | Acute Limb Ischaemia | Ankle-Brachial Pressure Index (ABPI) and Peripheral Vascular Disease | Peripheral Arterial Disease (PAD) | Abdominal Aortic Aneurysm (AAA) | Carotid Endarterectomy | Buerger's disease (Thromboangiitis obliterans) | Leriche syndrome (aortoiliac occlusive disease) |Acute Rhabdomyolysis |Hyperkalaemia |Acute Kidney Injury
Carotid Endarterectomy (CEA) is recommended for symptomatic carotid stenosis of 50–99% (NASCET criteria) or 70–99% (ECST criteria) in patients with recent TIA or non-disabling stroke (modified Rankin Scale ≤2), provided they are stable neurologically. Perform **urgently** - ideally as soon as possible and within **2 weeks** of the index event for maximum benefit (NICE NG128 1.2.4). Greatest absolute risk reduction occurs early after symptoms.
🧠 Evidence & Indications (NICE NG128 Compliant)
- CEA first described in the 1950s; randomised evidence from NASCET (1991) and ECST (1998) established benefit in symptomatic stenosis, reducing ipsilateral stroke risk.
- Strongest benefit: Symptomatic ≥70% stenosis (NASCET); absolute risk reduction (ARR) ~13–17% over 5 years vs medical therapy alone.
- Modest benefit: 50–69% stenosis (ARR ~7%; consider in men, recent symptoms, high-risk plaque features).
- No benefit: <50% stenosis, complete occlusion, or delayed intervention (>3–6 months).
- Timing critical: Benefit highest if CEA performed early (within days to 2 weeks of TIA/non-disabling stroke); delays reduce efficacy. Urgent referral via TIA clinic mandatory.
- Operator/centre factors: Perioperative stroke/death rate should be <6% (NICE standard); high-volume surgeons/centres preferred (audit via national registries e.g., UK National Vascular Registry).
- Stenosis measurement formula (NASCET): % stenosis = [1 - (minimal residual lumen diameter ÷ normal distal ICA diameter)] × 100. Reports must specify NASCET or ECST method (NG128 1.2.6).
- No routine CEA for asymptomatic stenosis (NG128 does not recommend; focus on BMT unless very high-risk features in specialist settings per other guidances).
🔬 Investigations
- First-line: Duplex ultrasound (carotid Doppler USS) - non-invasive, widely available, good sensitivity/specificity for ≥50% stenosis.
- Confirmatory/Planning: Contrast-enhanced MRA or CTA (preferred for detailed anatomy, plaque characteristics, and planning intervention).
- Consider dual-modality imaging (e.g., USS + MRA/CTA) before CEA to confirm degree and exclude tandem lesions (NG128 supports urgent carotid imaging in candidates).
- Avoid routine invasive DSA unless non-invasive imaging inconclusive.
- Brain imaging: MRI (diffusion-weighted) if needed to confirm ischaemic territory or exclude alternatives (NG128 1.2.2).
⚙️ The Procedure
- Anaesthesia: Local (preferred for neurological monitoring) or general.
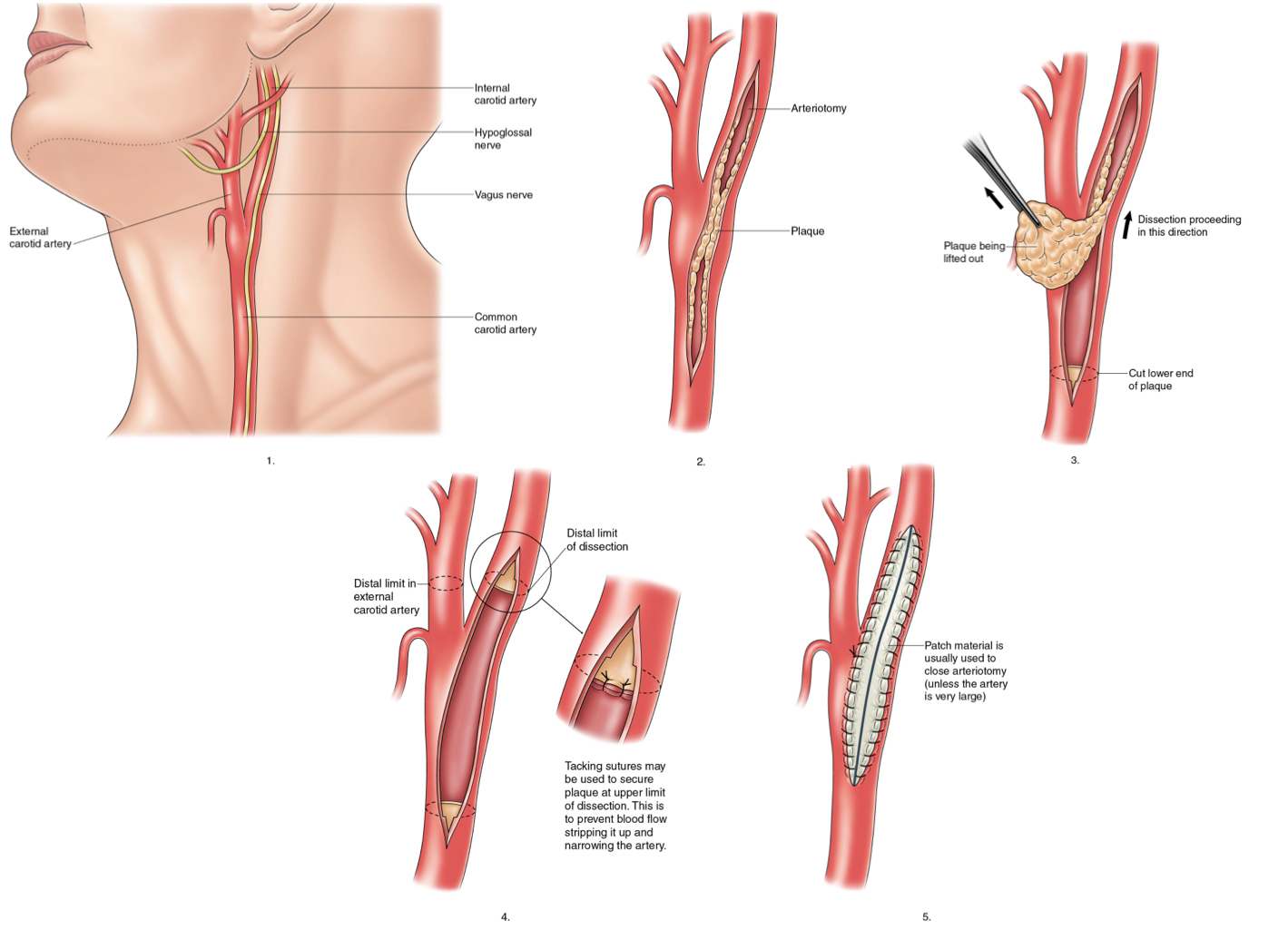
- Surgical steps: Neck incision; carotid exposure; clamping (test clamping or routine/selective shunting to maintain cerebral perfusion); arteriotomy; plaque endarterectomy; closure (primary suture or patch angioplasty - synthetic or vein - to reduce restenosis risk).
- Duration: Typically 60–120 minutes.
- Post-op: HDU/ICU monitoring for 24 hours (BP control to prevent hyperperfusion; neurological checks); most discharged day 1–2 if uncomplicated.
- Alternatives: Carotid artery stenting (CAS) considered in select high-surgical-risk patients (e.g., hostile neck, recent MI) per NICE IPG389 (2011; still current).
⚠️ Complications
| Complication | Incidence & Details | Management |
|---|---|---|
| Perioperative ischaemic stroke | ~2–6% (target <6%); embolic, thrombotic, or haemodynamic. | Urgent CT head (exclude ICH); CTA/MRA; antiplatelets ± re-exploration/endovascular rescue. |
| Cerebral hyperperfusion syndrome | 1–3%; days 3–10 post-op; headache, seizures, focal deficits, ICH due to impaired autoregulation. | Strict BP control (<140/90 mmHg or lower); anticonvulsants if seizures; neuroimaging (CT/MRI). |
| Restenosis | ~5–10% at 2–5 years; early (neointimal) or late (atherosclerotic). | Surveillance Duplex; medical optimisation; CAS or redo CEA if symptomatic. |
| Cranial nerve injury | 5–10% (hypoglossal, vagus, marginal mandibular, glossopharyngeal); usually transient. | Conservative; speech/swallow therapy; rarely permanent. |
| Post-op ICH | Rare (<1%); often related to hyperperfusion or antithrombotics. | Reverse anticoagulation; neurosurgical consult if large/mass effect. |
| Wound haematoma/infection | 1–5%; airway compromise possible. | Evacuation if expanding; antibiotics. |
| Myocardial infarction | 1–3%; higher in cardiac comorbidity. | Peri-op risk stratification (e.g., revised cardiac risk index). |
💊 Best Medical Therapy (Alongside or Instead of CEA – NG128 Compliant)
- Antiplatelet: Aspirin 75 mg daily (or clopidogrel 75 mg if intolerant); dual short-term in some high-risk cases.
- Lipid-lowering: High-intensity statin (e.g., atorvastatin 80 mg) targeting LDL <1.8 mmol/L.
- BP control: Target <130/80 mmHg (or lower if tolerated); ACEi/ARB first-line.
- Lifestyle: Smoking cessation (vital - halves recurrence risk); healthy diet, regular exercise, diabetes optimisation, alcohol moderation.
- Continue lifelong; BMT alone for non-surgical candidates or <50% stenosis.
📊 Secondary Stroke Prevention Benefit with CEA (Pooled NASCET/ECST Data)
| Severity of Stenosis (Symptomatic) | Relative Risk Reduction (5 yrs) | Absolute Risk Reduction (2 yrs approx.) | NNT (to prevent 1 stroke over 2–5 yrs) |
|---|---|---|---|
| Occluded | No role for CEA | - | - |
| 70–99% (NASCET) | ~65% | ~13–17% | ~6–8 |
| 50–69% (NASCET) | ~30% | ~7% | ~14 |
| <50% (NASCET) | No benefit | - | - |
💡 Key takeaway: Greatest benefit from CEA occurs early after TIA/non-disabling stroke (within 2 weeks; days if TIA-dominant). Reduced efficacy in women (lower ARR), ocular-only events (amaurosis fugax), lacunar strokes, contralateral occlusion, or delayed presentation. Always combine with aggressive BMT. Discuss in multidisciplinary team; refer urgently to vascular/stroke services meeting national standards.
📚 References (Current as of March 2026)
- NICE NG128 – Stroke and transient ischaemic attack in over 16s (2019; current) – Sections 1.2.3–1.2.6 on carotid imaging & urgent CEA.
- NASCET & ECST pooled analyses (Lancet/Rothwell et al.).
- NICE interventional procedures (e.g., IPG389 on CAS as alternative).
- 2023 NICE exceptional surveillance: No update needed for CEA recommendations.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery