
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Sprained Ankle ✅
Related Subjects: |Sprained Ankle |Achilles Tendon rupture |Acute Rotator Cuff Tear |Supraspinatus tendonitis |Ottawa rules for ankle and foot x-ray
🧠 An ankle sprain is an injury to the ankle ligaments, usually caused by twisting or inversion of the foot. Most are lateral ligament injuries, especially involving the anterior talofibular ligament (ATFL). The key clinical task is to exclude fracture, syndesmotic injury, tendon rupture and neurovascular compromise.
📖 About
- Common injury after twisting the ankle during sport, walking on uneven ground, falls or missteps.
- Usually affects the lateral ligament complex.
- The most commonly injured ligament is the anterior talofibular ligament.
- More severe inversion injuries may also damage the calcaneofibular ligament.
- Medial ankle sprains are less common because the deltoid ligament is stronger.
- High ankle sprain = injury to the syndesmosis between tibia and fibula.
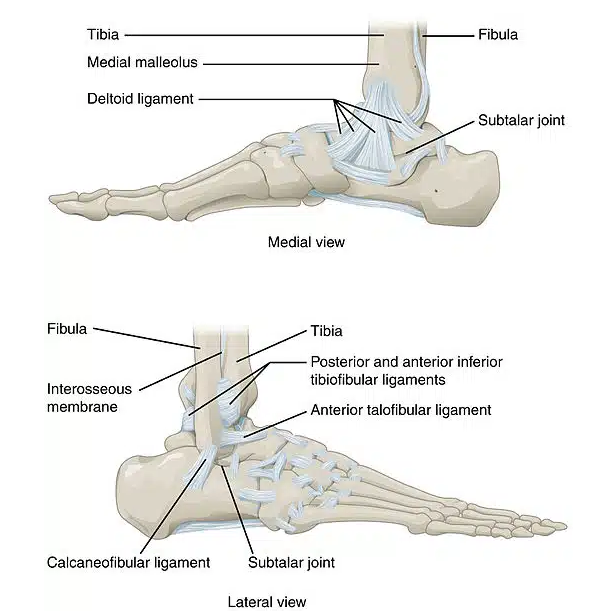
🧬 Relevant Anatomy
| Structure | Mechanism | Clinical clue |
|---|---|---|
| Anterior talofibular ligament
ATFL |
Inversion with plantarflexion | Most common sprain; tenderness anterior to lateral malleolus. |
| Calcaneofibular ligament
CFL |
More severe inversion injury | Tenderness inferior to lateral malleolus; instability may be greater. |
| Posterior talofibular ligament
PTFL |
Severe ankle trauma/dislocation | Rarely isolated; suggests major injury. |
| Deltoid ligament | Eversion injury | Medial ankle pain; consider associated fracture or syndesmotic injury. |
| Syndesmosis | External rotation / dorsiflexion injury | Pain above ankle joint, positive squeeze/external rotation test; slower recovery. |
⚙️ Mechanism
- 🌀 Inversion injury — foot rolls inwards; commonest mechanism.
- 🏃 Sports involving jumping, pivoting or sudden direction change.
- 🪨 Uneven ground or missing a step.
- ⚠️ External rotation injury may suggest syndesmotic/high ankle sprain.
- 🦴 Severe trauma or inability to weight bear raises concern for fracture.
🩺 Clinical Features
- Sudden ankle pain after twisting injury.
- Swelling around the lateral ankle, often developing rapidly.
- Bruising may appear over hours to days.
- Tenderness over ATFL/CFL region.
- Pain on weight bearing, walking, inversion or plantarflexion.
- Sense of instability or “giving way” in more severe sprains.
- Reduced range of movement due to pain and swelling.
🚩 Red Flags / Alternative Diagnoses
- Inability to weight bear immediately and in clinic/ED.
- Bony tenderness over posterior edge/tip of medial or lateral malleolus.
- Tenderness at the base of the 5th metatarsal.
- Tenderness over the navicular.
- Marked deformity or suspected dislocation.
- Neurovascular compromise: numbness, pallor, cold foot, weak pulses.
- Pain high above ankle joint → possible syndesmotic injury.
- Palpable Achilles gap or positive calf squeeze test → Achilles rupture.
- Severe persistent pain despite normal X-ray → consider occult fracture, osteochondral injury or tendon injury.
🧪 Examination
| Step | What to assess |
|---|---|
| Look | Swelling, bruising, deformity, wounds, foot position. |
| Feel | Lateral ligaments, medial ligament, malleoli, base of 5th metatarsal, navicular, Achilles tendon, proximal fibula. |
| Move | Active and passive dorsiflexion, plantarflexion, inversion and eversion. |
| Function | Ability to weight bear and walk four steps. |
| Neurovascular | Dorsalis pedis/posterior tibial pulses, capillary refill, sensation and movement. |
| Special tests | Anterior drawer/talar tilt if tolerated; squeeze/external rotation test if syndesmosis suspected. |
🦴 Ottawa Ankle Rules — When to X-ray
📌 Use the Ottawa ankle rules to decide whether an ankle or foot X-ray is needed after acute injury.
| X-ray area | Indication |
|---|---|
| Ankle X-ray |
Pain in the malleolar zone plus either:
|
| Foot X-ray |
Pain in the midfoot zone plus either:
|
🖼️ Imaging
- X-ray: if Ottawa ankle rules are positive, deformity is present, or fracture/dislocation is suspected.
- Ultrasound: not usually needed for simple ankle sprain, but may help assess tendon injury in selected cases.
- MRI: not routine in the acute phase of a simple ankle sprain; consider specialist-led MRI if persistent pain, suspected syndesmotic injury, osteochondral lesion, occult fracture, tendon injury, or failure to improve despite rehabilitation.
- Stress imaging: rarely needed acutely; usually specialist-led if chronic instability is suspected.
📊 Severity Grading
| Grade | Injury | Clinical picture | Recovery |
|---|---|---|---|
| Grade I | Ligament stretch / microscopic tear | Mild pain, minimal swelling, able to weight bear. | Usually days to 2 weeks. |
| Grade II | Partial ligament tear | Moderate pain, swelling, bruising, painful walking, some instability. | Often 2–6 weeks. |
| Grade III | Complete ligament rupture | Severe swelling/bruising, marked instability, difficulty weight bearing. | Often 6–12 weeks or longer; may need specialist review. |
🏥 Initial Management — PRICE / POLICE
- Protection: avoid painful activities and further injury for the first 48–72 hours.
- Relative rest: avoid complete immobilisation unless severe injury or fracture is suspected.
- Optimal loading: begin gentle movement and weight bearing as pain allows.
- Ice: may help pain and swelling in the first 48–72 hours; wrap ice pack in a towel to avoid ice burns.
- Compression: elastic bandage or ankle support can reduce swelling.
- Elevation: raise ankle above heart level when resting.
- Analgesia: paracetamol ± NSAID if appropriate; consider topical NSAID.
- Rehabilitation: progressive range-of-movement, strengthening and balance/proprioception exercises reduce recurrent sprain risk.
🚶 Rehabilitation
| Phase | Goals | Examples |
|---|---|---|
| Early phase
0–3 days |
Reduce pain/swelling, protect injury, maintain gentle movement. | Elevation, compression, ankle circles, gentle dorsiflexion/plantarflexion, weight bear as tolerated. |
| Recovery phase
3 days–2 weeks |
Restore range of movement and normal walking. | Walking practice, calf stretches, resisted band exercises, gradual return to daily activity. |
| Strength / balance phase
2–6 weeks |
Improve strength, proprioception and stability. | Single-leg stance, wobble board, heel raises, resisted eversion/inversion. |
| Return to sport | Restore agility, power and confidence. | Hopping, cutting, running drills, sport-specific training; ankle brace/taping may reduce recurrence. |
📅 Follow-Up / Referral
- Mild sprain: self-care advice, early mobilisation and safety-netting.
- Moderate sprain: consider physiotherapy, ankle support and review if not improving.
- Severe sprain: fracture clinic, MSK or physiotherapy review depending on local pathway.
- Urgent referral: fracture/dislocation, neurovascular compromise, open injury, suspected syndesmotic injury, Achilles rupture, tendon injury, or inability to weight bear with concerning signs.
- Persistent symptoms: review if pain, swelling, instability or inability to return to function persists beyond 4–6 weeks.
⚠️ Complications
- Chronic ankle instability and recurrent sprains.
- Persistent swelling and stiffness.
- Peroneal tendon injury.
- Osteochondral lesion of the talus.
- Missed fracture, especially base of 5th metatarsal, lateral process of talus, posterior malleolus or navicular.
- Complex regional pain syndrome, rarely.
💡 Clinical Pearls
- Most ankle sprains are lateral ligament injuries from inversion.
- Use Ottawa ankle rules to decide on X-ray after acute injury.
- Ability to walk does not fully exclude serious injury, but inability to weight bear is a key imaging trigger.
- High ankle sprains hurt above the ankle joint and recover more slowly.
- Early functional rehabilitation reduces stiffness and recurrent sprain risk.
- Persistent pain after a “sprain” needs reassessment for occult fracture, syndesmotic injury or osteochondral lesion.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery