
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Autoimmune Liver Disease Table ✅
Related Subjects: |Chronic liver disease |Cirrhosis |Alkaline phosphatase (ALP) |Liver Function Tests |Ascites Assessment and Management |Budd-Chiari syndrome |Autoimmune Hepatitis |Primary Biliary Cirrhosis |Primary Sclerosing Cholangitis |Wilson disease |Hereditary Haemochromatosis |Alpha-1 Antitrypsin (AAT) deficiency |Non alcoholic steatohepatitis (NASH) |Spontaneous Bacterial Peritonitis |Alcoholism and Alcoholic Liver Disease |Hepatitis C |Autoimmune Liver Disease Table
🧠 Introduction
Autoimmune liver diseases (AILDs) comprise a spectrum of chronic liver disorders where the body’s immune system targets hepatocytes or biliary epithelium, leading to inflammation, cholestasis, fibrosis, and eventually cirrhosis if untreated. These include Autoimmune Hepatitis (AIH), Primary Biliary Cholangitis (PBC), Primary Sclerosing Cholangitis (PSC), and overlap syndromes. Early recognition is crucial to prevent long-term complications such as cirrhosis, hepatocellular carcinoma, portal hypertension, and liver failure.
🧬 Initial Pathophysiology
- Immune-mediated attack against hepatic tissue or bile ducts triggers chronic inflammation.
- In AIH, loss of tolerance to hepatocyte antigens → T-cell mediated cytotoxicity and plasma cell infiltration → interface hepatitis.
- In PBC, autoimmune destruction of intrahepatic bile ducts → cholestasis, bile acid accumulation, and progressive fibrosis.
- In PSC, immune-mediated inflammation causes multifocal bile duct strictures → cholestasis, recurrent cholangitis, and eventual secondary biliary cirrhosis. Strong association with ulcerative colitis suggests gut-liver immune cross-talk.
- Chronic inflammation activates stellate cells → fibrosis → cirrhosis over years; persistent cholestasis impairs fat-soluble vitamin absorption and bone health.
💡 Clinical takeaway: Understanding the underlying immune-mediated injury explains why immunosuppression benefits AIH, while PBC/PSC require long-term cholestasis management and monitoring for complications. Early recognition and serological testing guide appropriate therapy and referral.
🧠 Autoimmune Liver Disease (UK)
| Condition | How to recognise (features • labs • imaging/biopsy) | First-line & follow-up (UK / NICE-aligned) |
|---|---|---|
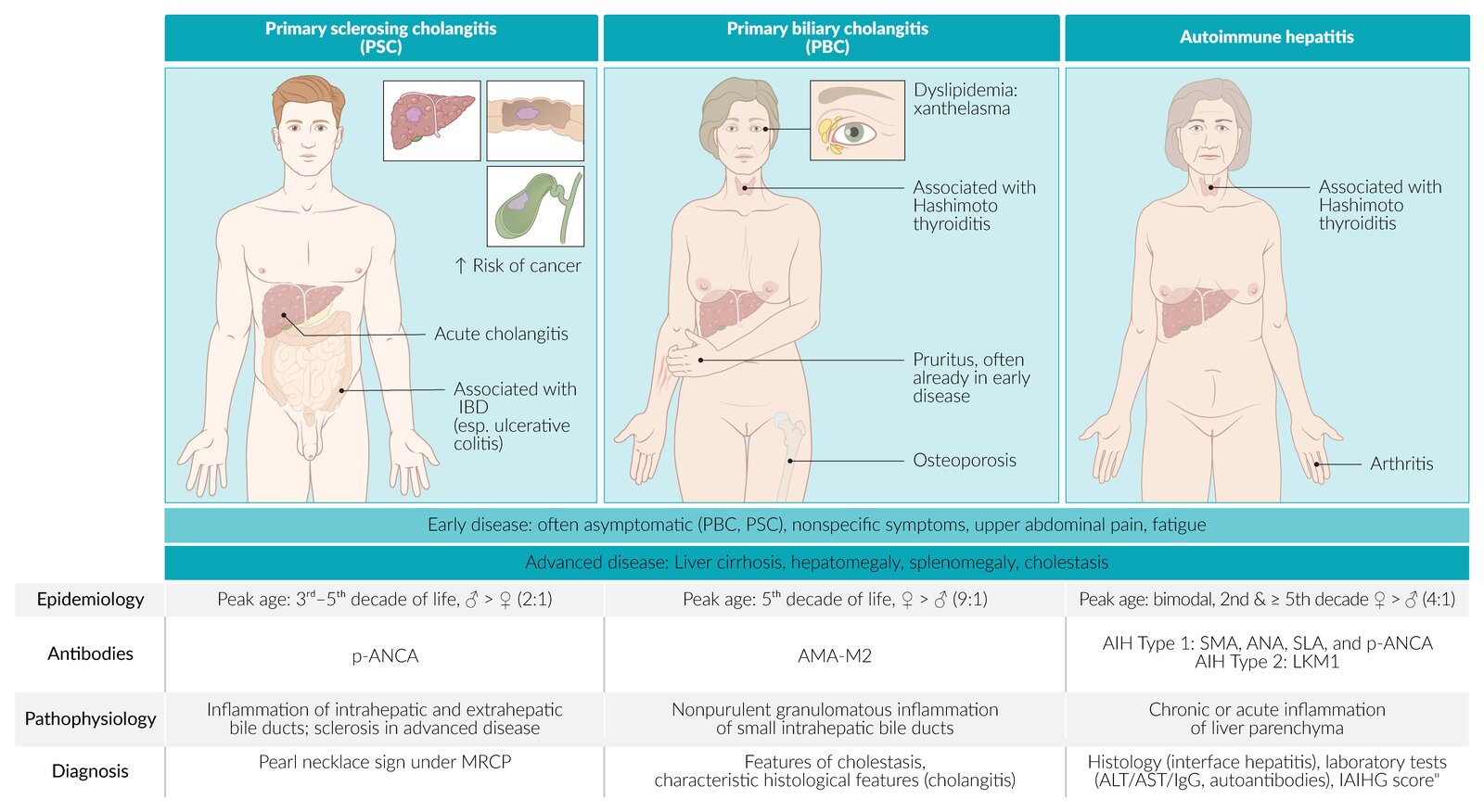
| 🩷 Autoimmune Hepatitis (AIH) | Hepatitic LFTs (ALT/AST ≫ ALP), fatigue, jaundice; can be acute or severe. ↑ IgG; ANA/SMA (type 1), anti-LKM1 (type 2), anti-SLA/LP. Liver biopsy: interface hepatitis with plasma cells; exclude viral hepatitis. | Prednisolone → taper + azathioprine (or MMF if AZA-intolerant). Aim: normal ALT/AST & IgG; monitor q3–6 months. Cirrhosis → HCC surveillance (US ± AFP 6-monthly). Advise vaccination (hep A/B, influenza, pneumococcal). |
| 💚 Primary Biliary Cholangitis (PBC) | Cholestatic pattern (ALP ≫ ALT), pruritus, fatigue, xanthelasma. ↑ IgM; AMA-M2 (~95%); if AMA-negative: ANA gp210/sp100. Imaging to exclude obstruction; biopsy if atypical. | UDCA 13–15 mg/kg/day; check 12-mo biochemical response. Non-responders → consider obeticholic acid* or bezafibrate† under specialist care. Pruritus: cholestyramine → rifampicin → naltrexone. DEXA for bone health; fat-soluble vitamins; HCC surveillance if cirrhotic. |
| 🌀 Primary Sclerosing Cholangitis (PSC) | Often men 30–40 yrs; strong UC link; cholestatic LFTs, pruritus, recurrent cholangitis. p-ANCA common (non-specific); check IgG4 to exclude IgG4-SC. MRCP: multifocal strictures “beading”; biopsy if small-duct disease suspected. | No proven disease-modifying drug. Treat complications: cholangitis (antibiotics), dominant strictures (ERCP ± stent). Transplant if advanced/intractable pruritus. Cancer risks: cholangiocarcinoma, gallbladder, colorectal (if IBD) → colonoscopy 1–2 yearly; annual gallbladder US; follow local CCA protocols. |
| 🔗 Overlap (AIH–PBC / AIH–PSC) | Mixed cholestatic + hepatitic LFT pattern; combined serology (AMA + ↑IgG/ANA/SMA). Biopsy often needed to confirm. | Combine therapies: steroids ± AZA for AIH component + UDCA for cholestasis. Tailor surveillance to both diseases; specialist follow-up essential. |
* Obeticholic acid contraindicated in decompensated cirrhosis (Child-Pugh B/C). † Bezafibrate off-label in the UK; specialist use for non-responders.
🧭 Practical UK Notes (Primary Care / GP)
- 📉 Targets: ALT/AST normalisation (AIH), ALP & bilirubin fall (PBC), symptom control (PSC).
- 🔁 Monitoring: LFTs & IgG/ALP q3–6 months; bone health (DEXA); fat-soluble vitamins if advanced cholestasis.
- 🧪 Before AZA: TPMT/NUDT15 testing; counsel on sun protection, cytopenias, infection risk.
- 🧻 Pruritus management: cholestyramine (separate from other meds by 4 h), rifampicin, naltrexone, sertraline (specialist if refractory).
- 🧪 PSC + IBD: colonoscopic surveillance 1–2 yearly from diagnosis, regardless of IBD duration.
- 🏥 Transplant referral: decompensated cirrhosis, intractable pruritus (PBC/PSC), recurrent cholangitis (PSC), acute severe AIH non-responsive to therapy.
- 💉 Vaccinations: hep A/B, influenza, pneumococcal (especially if immunosuppressed).
- 🧾 Patient education: chronic disease counselling, lifestyle advice, adherence to therapy, monitoring for complications.
💡 Teaching tip: AIH responds to immunosuppression; PBC/PSC are cholestatic, slowly progressive, and require long-term monitoring. Always check for overlap syndromes. Early referral for transplant assessment if decompensation occurs.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery