
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Pelvic fractures
Related Subjects: |Supracondylar Femur Fractures |Supracondylar Humerus Fractures |Femoral fractures |Fractured Tibia and Fibula |Pelvic fractures |Fractured Neck of Femur |Fractured Shaft Femur |Supracondylar Femur Fractures |Femoral fractures and Injuries
Pelvic Fractures 🦴🚨 are high-risk injuries often associated with major trauma, haemorrhage, and multi-organ injury. 👉 Mortality ≈10% in closed fractures, up to 50% in open fractures. Always consider associated injuries and hidden blood loss → involve the major trauma centre early.
📖 About
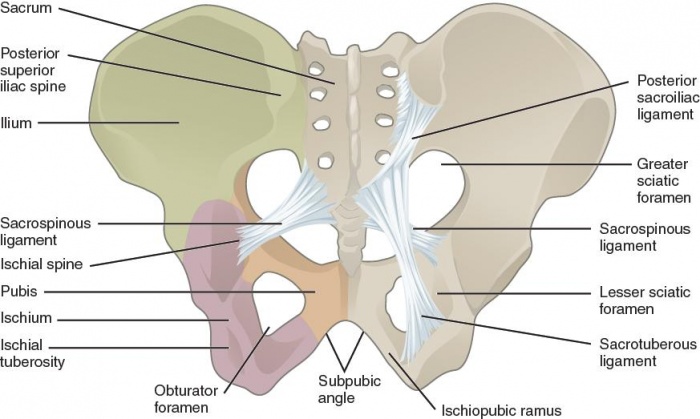
- Pelvis = bony ring formed by sacrum, SI joints, innominate bones, and pubic symphysis.
- Fractures usually occur in ≥2 places due to ring structure.
- Mechanism: high-energy trauma (RTA, fall from height, crush). Low-energy fragility fractures in elderly/osteoporotic patients.
⚙️ Aetiology
- High force → RTA, falls, crush injuries.
- Low force → osteoporotic or pathological fractures.
- Structures at risk: bladder, urethra, vessels, rectum, uterus/vagina.
🩺 Clinical Features
- Shock from haemorrhage (may be hidden retroperitoneal).
- Severe pelvic/hip pain, bruising, swelling.
- Urethral injury signs: blood at meatus, high-riding prostate (on PR).
- PV/PR bleeding may indicate vaginal/rectal injury.
- Always assess for other trauma (head, chest, abdomen, spine).
🔎 Predictors of Major Haemorrhage
- Hct < 30% 📉
- HR > 130 bpm ❤️🔥
- Displaced obturator ring fracture
- Wide pubic symphyseal diastasis
📊 Tile Classification
| Type A | Stable: avulsion fractures, isolated pubic ramus, iliac wing fractures. Often low-energy, muscle avulsion (e.g. AIIS → rectus femoris, ASIS → sartorius, ischial tuberosity → hamstrings). |
| Type B | Rotationally unstable but vertically stable. B1 = “open book” (AP compression). B2 = ipsilateral compression (overriding pubic bones). B3 = contralateral compression (pubic rami fracture one side + SI compression other side). |
| Type C | Rotationally + vertically unstable. Ring disrupted in ≥2 places. Massive blood loss, high mortality. C1 unilateral, C2 bilateral, C3 with acetabular involvement. |
🧾 Simple Classification
- Stable: single break, minimal bleeding, bones remain aligned.
- Unstable: ≥2 breaks, moderate–severe bleeding, deformity.
⚠️ Complications
- Massive haemorrhage, intrapelvic compartment syndrome.
- Bladder, urethral, vaginal, rectal injuries.
- Venous thromboembolism.
- Sexual dysfunction, impotence.
- Chronic instability, deformity, pain.
- Infection/osteomyelitis (esp. open fractures).
🧪 Investigations
- Bloods: FBC, U&E, coagulation, group & crossmatch.
- Urinalysis (haematuria → bladder/urethral injury).
- X-ray: AP pelvis (trauma screen).
- CT: pelvic inlet/outlet, evaluate associated injuries.
- Retrograde urethrogram if urethral injury suspected.
- Angiography: for ongoing bleeding (>0.5 units/hr) → embolisation.
💊 Management
- Initial: ATLS protocol, balanced resuscitation, analgesia.
- Pelvic binder: apply if haemodynamic instability suspected → reduces pelvic volume, promotes clot formation. Keep on until definitive management.
- Do not roll in unstable B/C fractures → use straight lift with ≥4 helpers.
- Avoid urethral catheter if blood at meatus/high-riding prostate → consider suprapubic catheter.
- Open wounds: IV antibiotics, tetanus, urgent debridement. May need colostomy if bowel involved.
- Definitive:
- Type A: usually conservative → analgesia, rest, mobilisation with aids. Fixation if acetabulum involved.
- Type B/C: external fixation (pins + frame) or internal fixation (plates/screws). Consider angiography/embolisation if persistent bleeding.
📌 OSCE / Exam Pearls
- Pelvic fracture = assume massive blood loss until proven otherwise.
- Blood at urethral meatus 🚨 → do NOT catheterise → retrograde urethrogram first.
- Apply pelvic binder early in shocked trauma patient with pelvic injury suspicion.
- Stable vs unstable classification is high-yield in exams.
📚 References
- ATLS®: Advanced Trauma Life Support, 10th edition.
- BOAST Guidelines: Management of Pelvic Fractures.
- Rockwood & Green’s Fractures in Adults, 9th edition.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery