Related Subjects:
|Antepartum haemorrhage
|Postpartum haemorrhage
|Acute Haemorrhage
|Placenta praevia
|Placenta abruption
|Anti-D immunoglobulin
👶 About Multiple Pregnancies
- Incidence: Twins occur in ~1 in 80 pregnancies; triplets in ~1 in 6,400 (80 × 80). Higher-order multiples (quadruplets and beyond) are rare and usually linked to assisted reproduction (IVF, ovulation induction).
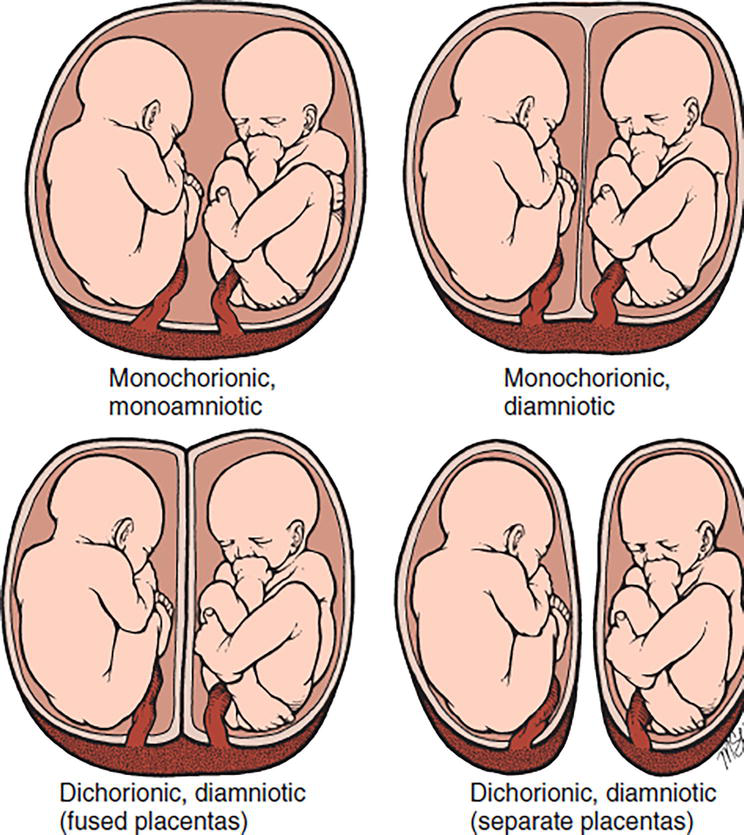
- Monozygotic (Identical) Twins:
- Arise from splitting of a single fertilised egg → genetically identical, same sex.
- Monochorionic: One placenta, ↑ risk of Twin-to-Twin Transfusion Syndrome (TTTS).
- Dichorionic: Two placentas, lower risk of transfusion complications, better prognosis.
- Dizygotic (Fraternal) Twins: Two separate eggs + sperm. Always dichorionic. Can be same or different sex.
- Key Risk in Monochorionic Twins: Shared vessels → risk of TTTS, selective IUGR, and twin anaemia–polycythaemia sequence (TAPS).
⚠️ Risks in Twin & Multiple Pregnancies
- ⬆️ Stillbirth & Neonatal Death: Higher than in singleton pregnancies due to prematurity, low birthweight, and complications.
- 🫁 Preterm Labour: >50% of twins deliver <37w; nearly all triplets <35w → ↑ risk of RDS, NEC, IVH.
- 🤢 Hyperemesis gravidarum: More common/severe due to high hCG levels.
- 🩸 Pre-eclampsia: 2–3× higher risk → monitor BP and proteinuria closely.
- 🩻 Anaemia: Increased maternal iron demand → often needs supplementation.
- 🧬 Congenital abnormalities: Particularly ↑ in monozygotic twins.
- 📉 IUGR: Common due to placental sharing or discordant growth.
- 🫄 Malpresentation & cord prolapse: Space constraint → breech/transverse frequent.
- 🧠 Cerebral Palsy: Risk ~3–5× higher, mostly due to prematurity/hypoxia.
➕ Additional Complications
- TAPS (Twin Anaemia–Polycythaemia Sequence): Tiny vascular anastomoses → one twin anaemic, the other polycythaemic (no liquor discordance unlike TTTS).
- Selective IUGR (sIUGR): One twin small, the other normal; surveillance and delivery timing are challenging.
- Vanishing Twin Syndrome: Early loss of one twin, often absorbed before recognition.
- High-Risk Care: Specialist maternal-fetal medicine input with frequent growth scans + Dopplers is essential.
🩺 Management Strategies
- Ultrasound Monitoring:
- Monochorionic: scans every 2 weeks from 16w (to detect TTTS/TAPS).
- Dichorionic: every 4 weeks.
- Specialised Antenatal Care: Early booking, serial BP & urine checks, GDM screening, nutritional optimisation (iron, folate, calcium).
- Nutrition: ↑ calorie & protein needs; iron and folate supplementation recommended.
- Activity: Avoid excessive exertion; some women may need reduced activity in late pregnancy.
- Delivery Planning:
- Twins: C-section if first twin breech/transverse; vaginal delivery can be considered if first twin cephalic + experienced obstetric team.
- Triplets/higher: usually C-section due to logistics/risks.
📌 Exam Pearls
- TTTS only occurs in monochorionic twins → look for liquor discordance.
- Vanishing twin explains early pregnancy bleeding or scan changes.
- TAPS is harder to detect → middle cerebral artery Dopplers are key.
- Any multiple pregnancy = consultant-led, high-risk pathway (RCOG Green-top guideline No. 51).
