Spinal Cord Injury / Malignant Spinal Cord Compression (MSCC)
Related Subjects:
| Osteoporosis
⚠️ Malignant Spinal Cord Compression (MSCC) is a medical, oncological, and surgical emergency.
⏱️ Immediate treatment is crucial to prevent paralysis and sphincter dysfunction.
💊 Dexamethasone 16 mg should be given immediately if MSCC is suspected (unless contraindicated).
ℹ️ About
- 🚨 MSCC = emergency requiring urgent diagnosis + treatment.
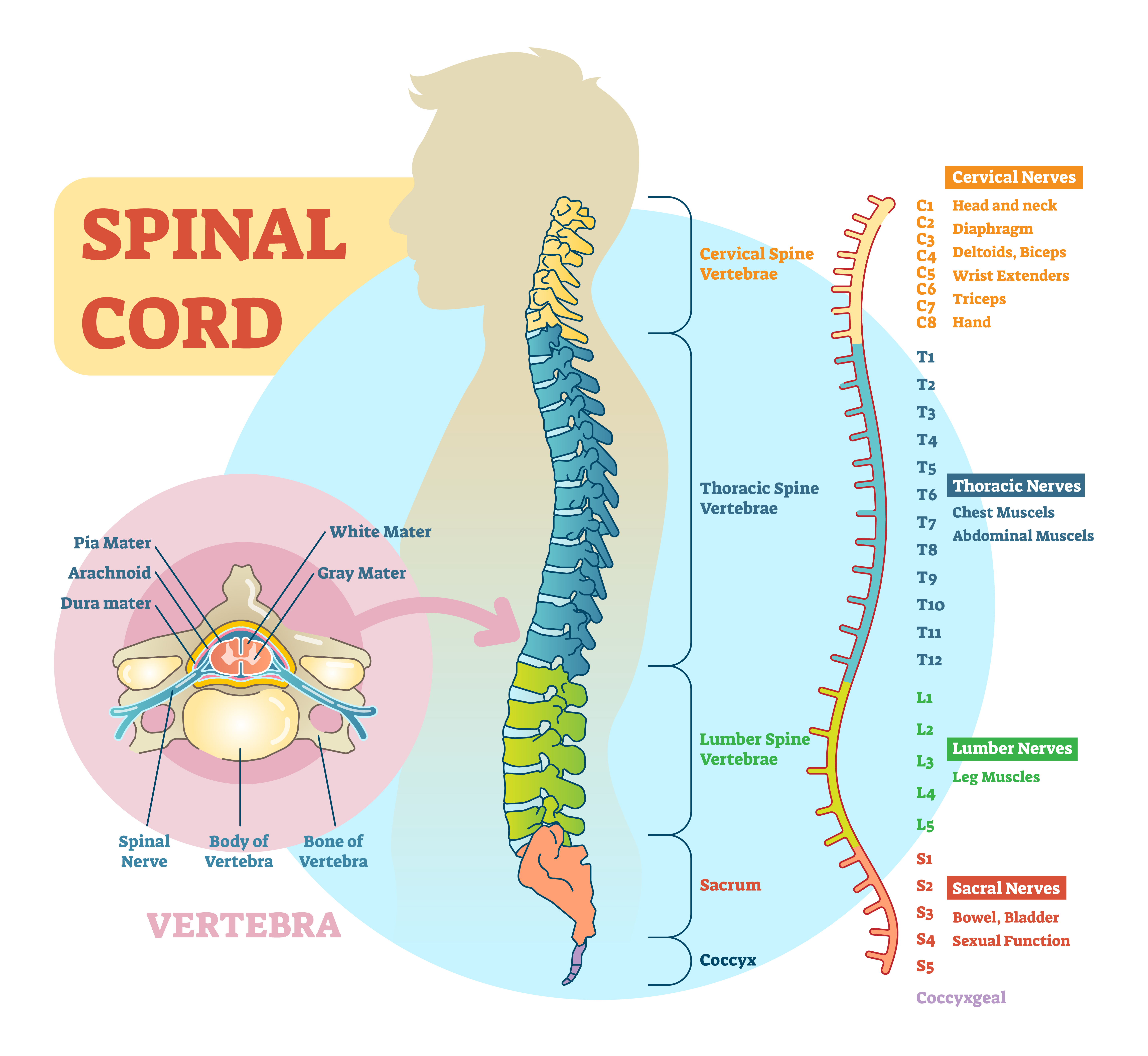
- 🧠 Spinal cord ends at L1 → lesions above cause UMN signs; Cauda equina below L1 causes LMN signs.
- 🎯 Goal = preserve mobility, bladder/bowel function, and quality of life.
🧾 Causes
- 💥 Trauma with fracture fragments.
- 🩸 Epidural haematoma (trauma, anticoagulation).
- 🦠 Epidural abscess (staph aureus common).
- 💿 Central disc prolapse (massive herniation).
- 🎗️ Metastases (prostate, breast, lung, lymphoma, myeloma, melanoma, renal cell carcinoma).
🩺 Clinical Features
- 💢 Severe back or radicular pain (often nocturnal, not relieved by rest).
- 🦵 UMN signs: sensory level, spasticity, hyperreflexia, Babinski sign.
- 🧤 Radiculopathy: asymmetric numbness, tingling, root pain.
- 🚽 Sphincter symptoms: retention, incontinence, loss of anal tone.
- 🍑 Cauda equina syndrome: saddle anaesthesia, LMN leg weakness, areflexia.
- 🎗️ Often background of malignancy (prostate, breast, lung, myeloma).
🔎 Investigations
- 🧪 Bloods: FBC, U&E, LFTs, ESR/CRP, ALP, PSA, paraproteins, Bence-Jones protein.
- 🖥️ Imaging:
- 🎯 MRI whole spine within 24h (gold standard).
- 🩻 CT if MRI contraindicated/unavailable.
- 🫁 CT chest/abdomen/pelvis for staging.
- 👩 Mammogram if breast primary suspected.
💊 General Management
- 📞 Immediate referral to neurosurgery & oncology.
- 🛏️ Bed rest & log-rolling until stability confirmed.
- 💊 Adequate analgesia (often opioids) + laxatives.
- 🚽 Bladder: catheterisation / ISC training if retention.
- 🍽️ Bowel care:
– Above T12/L1 → spastic bowel (reflex intact).
– Below T12/L1 → flaccid bowel (manual evacuation often required).
- 💉 VTE prophylaxis: very high risk.
🎗️ Specific MSCC Management
- 💊 Dexamethasone 16 mg OD (or 8 mg BD) + PPI cover.
- ☢️ Radiotherapy: first-line for most, especially radiosensitive tumours (myeloma, lymphoma, breast, prostate, small-cell lung).
- 🔪 Surgery: urgent decompression ± fixation if fit, single level, or unstable spine.
- 💉 Chemotherapy: chemosensitive tumours (lymphoma, germ cell, neuroblastoma).
- 🩺 Palliative care: if prognosis very poor or paraplegic >24h without pain.
🦴 Spinal Stability Factors
- 📍 Site: cervical least stable; thoracic more stable (rib support).
- 📉 Extent of vertebral body involvement → risk of collapse.
- ⚖️ Comorbidity: osteoporosis, steroids, frailty → weaker bones.
- 🔪 Surgery: decompression may destabilise, fixation often needed.
📊 Prognosis (Median Survival after MSCC)
- 🫁 Lung cancer – ~32 days.
- 🍏 Prostate cancer – ~114 days.
- 🎗️ Breast cancer – ~74 days.
- 🧬 Lymphoma – ~226 days.
- 🦴 Myeloma – ~374 days.
- ❓ Unknown primary – ~41 days.
📝 Exam / OSCE Pearls
- 🧠 Distinguish UMN (cord) vs LMN (cauda equina).
- 💊 Dexamethasone 16 mg = first step in suspected MSCC.
- ⏱️ Always mention urgent MRI whole spine within 24h.
- ☢️ Radiotherapy is mainstay; surgery if instability or single lesion.
- 📌 Ask about red-flag symptoms: saddle anaesthesia, sphincter disturbance, progressive weakness.
📚 References
