
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Diaphragm
Related Subjects: |AP of the Oesophagus |AP of the Diaphragm |AP of the Large Bowel (Colon, Rectum, Anal Canal) |AP of Small Bowel |AP of the Biliary system |AP of the Bone Marrow |AP of the Eye |AP of the Pharynx |AP of the Larynx |AP of the Ear |AP of the Nose |AP of Male Genitalia |AP of the Breast |AP of the Stomach |AP of the Rectum |AP of the Spleen
The diaphragm is a dome-shaped, musculotendinous partition separating the thoracic and abdominal cavities. It is the primary muscle of respiration, generating negative intrathoracic pressure for inspiration, and it also serves as a key pressure regulator (coughing, vomiting, defecation, parturition) and an important contributor to the anti-reflux barrier at the gastro-oesophageal junction. Functionally, it is both a respiratory pump and a postural/pressure muscle.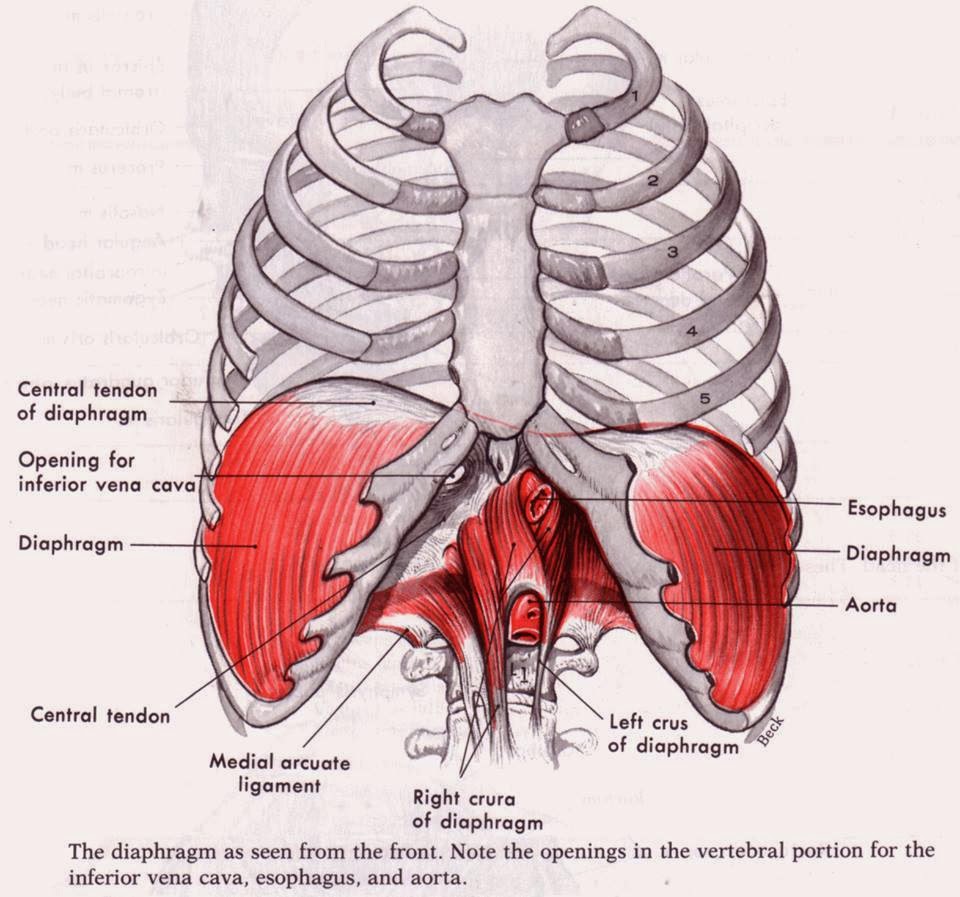
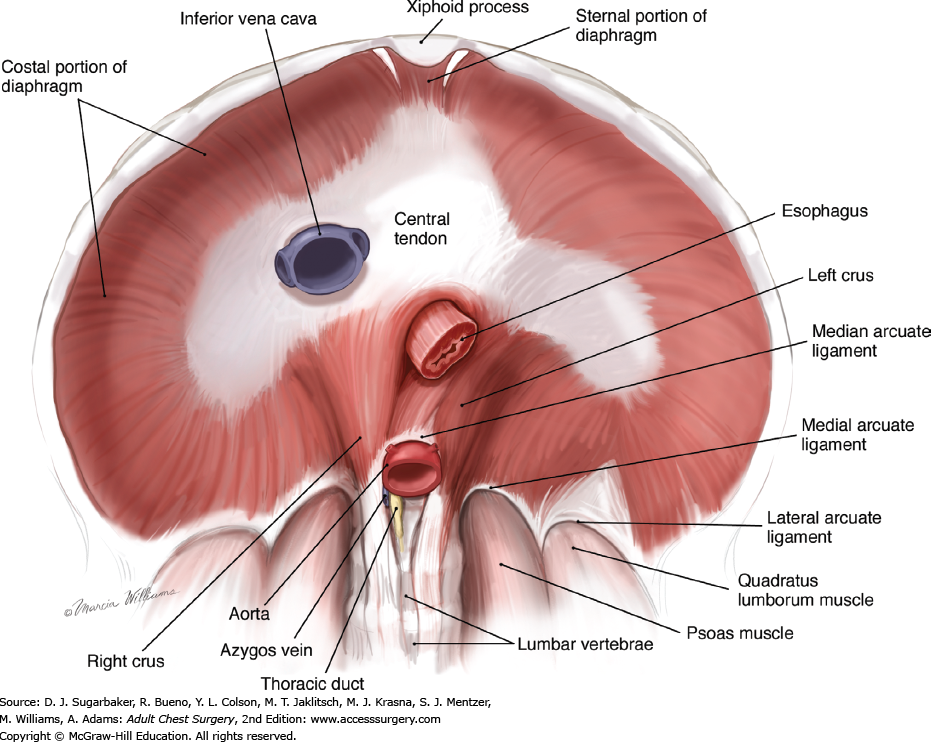
1️⃣ Anatomy: Structure & Attachments
- 🛑 Dome shape: Convex superior (thoracic) surface and concave inferior (abdominal) surface.
- Right hemidiaphragm is usually higher than the left due to the liver.
- The dome rises and falls with breathing, posture, and abdominal pressure.
- ⭐ Central tendon: A non-contractile aponeurosis where muscle fibres converge.
- Fused to the fibrous pericardium → explains why diaphragmatic movement influences cardiac position and why central irritation can feel “in the chest”.
- During contraction, the central tendon descends, increasing thoracic volume.
- 💪 Muscular portions (origins):
- Sternal part: arises from the posterior xiphoid process.
- Costal part: arises from inner surfaces of ribs 7–12 and their costal cartilages (largest portion).
- Lumbar part: arises via the crura and arcuate ligaments:
- Right crus: typically larger/longer; attaches to upper lumbar vertebrae and contributes to the oesophageal “pinch-cock” effect.
- Left crus: smaller; attaches to upper lumbar vertebrae.
- Median arcuate ligament: arches over the aorta.
- Medial arcuate ligament: arches over psoas major.
- Lateral arcuate ligament: arches over quadratus lumborum.
- 🧱 Surfaces & coverings:
- Superior surface: covered by diaphragmatic pleura.
- Inferior surface: covered by peritoneum (except where directly related to the liver via bare area relationships).
- Major relations:
- Right: liver.
- Left: stomach and spleen.
- Posterior: kidneys and adrenal glands.
🚪 Major Openings (Hiatuses) & What Passes Through
The diaphragm is pierced by several openings that transmit major vessels and the oesophagus. These openings are clinically important for hernias, reflux, and the spread of infection/malignancy between thorax and abdomen.
- 🧃 Caval opening (T8): IVC (+ right phrenic nerve branches).
- Located in the central tendon → it widens during inspiration, aiding venous return to the heart.
- Mnemonic: “Vena cava at 8”.
- 🥤 Oesophageal hiatus (T10): oesophagus + vagus nerves (anterior and posterior vagal trunks) ± oesophageal vessels/lymphatics.
- Formed mainly by the right crus → diaphragmatic fibres contribute to the anti-reflux barrier.
- Mnemonic: “Eggs at 10”.
- 🅰️ Aortic hiatus (T12): aorta + thoracic duct ± azygos/hemiazygos vein.
- Passes posterior to the diaphragm (beneath median arcuate ligament) → less affected by diaphragmatic contraction.
- Mnemonic: “Aorta at 12”.
- Mnemonic: “I 8 10 Eggs At 12” 🥚 (IVC T8, Oesophagus T10, Aorta T12).
2️⃣ Innervation (Motor + Sensory)
- 💡 Phrenic nerves (C3–C5): motor supply to the diaphragm and sensory to the central diaphragm, pericardium, and mediastinal pleura.
“C3, 4, 5 keep the diaphragm alive.” - 🌐 Peripheral sensory: lower intercostal nerves provide sensory input to the peripheral diaphragm and costal pleura/peritoneum.
- Referred pain: central diaphragmatic irritation → shoulder tip pain (C3–C5 dermatomes) via phrenic nerve afferents.
3️⃣ Blood Supply & Venous Drainage
- Arterial:
- Pericardiophrenic and musculophrenic arteries (branches of internal thoracic artery).
- Superior phrenic arteries (from thoracic aorta).
- Inferior phrenic arteries (from abdominal aorta; major inferior supply).
- Venous drainage: drains to brachiocephalic veins (via pericardiophrenic), azygos system, and IVC (via inferior phrenic veins).
⚙️ Physiology of the Diaphragm
🌬️ 1. Ventilation Mechanics (How it moves air)
In quiet breathing, the diaphragm is responsible for the majority of inspiratory work. When it contracts, muscle fibres shorten and the dome descends, increasing thoracic volume. This lowers intrathoracic pressure and draws air into the lungs. Expiration at rest is largely passive due to elastic recoil of the lungs and chest wall.
- Inspiration: diaphragm contracts and flattens → ↑ thoracic volume → ↓ intrathoracic pressure → air flows in.
- Expiration (quiet): diaphragm relaxes → domes rise → elastic recoil drives airflow out.
- Accessory recruitment: in respiratory distress, accessory muscles assist, but diaphragmatic fatigue can be a key limiting factor.
- Zone of apposition: the diaphragm apposes the lower rib cage; contraction expands the lower ribs (“bucket-handle” contribution) improving ventilation efficiency.
🩸 2. The Respiratory Pump (Venous return & lymph flow)
- Venous return: inspiration makes intrathoracic pressure more negative and increases intra-abdominal pressure → “squeezes” abdominal veins while “sucking” blood toward the heart.
- IVC effect: the caval opening in the central tendon widens on inspiration, facilitating IVC flow.
- Lymphatics: pressure oscillations also promote thoracic duct and lymph flow.
💥 3. Pressure Regulation (Posture & “strain” manoeuvres)
The diaphragm is a core muscle. By contracting against a closed glottis or coordinated abdominal wall contraction, it raises intra-abdominal pressure and stabilises the spine. This underpins coughing, vomiting, defecation, urination, and childbirth.
- Valsalva manoeuvre: forced expiration against a closed glottis increases intrathoracic pressure, affecting venous return and blood pressure (important in syncope physiology and some arrhythmia termination strategies).
- Cough: deep inspiration then forced expiration against a briefly closed glottis generates high expiratory flow to clear secretions.
- Core stabilisation: diaphragm + pelvic floor + abdominal wall create a pressure cylinder supporting posture and load transfer.
🛡️ 4. Anti-reflux Function (GOJ physiology)
- The right crus forms a dynamic sling around the oesophageal hiatus; diaphragmatic contraction augments LES pressure (“external sphincter”).
- A short intra-abdominal oesophagus and the angle of His contribute further to reflux prevention.
- Hiatus hernia disrupts this anatomy, weakening the barrier and predisposing to reflux symptoms and oesophagitis.
📊 Clinical Pearls
- 📌 Hiatal hernia: sliding (common, reflux) vs para-oesophageal/rolling (risk of strangulation/volvulus).
- 📌 Phrenic nerve palsy: raised hemidiaphragm on CXR; may cause exertional dyspnoea, orthopnoea, and reduced vital capacity (especially supine).
- 📌 Referred pain: diaphragmatic pleurisy, subphrenic abscess, or blood/air under diaphragm → shoulder tip pain (C3–C5).
- 📌 Hiccups: involuntary diaphragmatic spasms due to irritation of phrenic/vagal pathways or gastric distension; persistent hiccups warrant systemic review.
- 📌 Trauma: diaphragmatic rupture (often left-sided) can allow herniation of abdominal contents into the thorax.
📝 Summary
The diaphragm is a dome-shaped musculotendinous sheet with sternal, costal, and lumbar (crural) attachments converging on a central tendon. It has three key openings (IVC T8, oesophagus T10, aorta T12) and is powered by the phrenic nerves (C3–C5). Physiologically, diaphragmatic contraction is the main driver of inspiration, enhances venous return via the respiratory pump, supports posture and pressure-dependent functions, and strengthens the anti-reflux barrier at the oesophageal hiatus. Many clinical signs-shoulder tip referred pain, raised hemidiaphragm, and reflux with hiatal hernia-are direct consequences of this anatomy–function relationship.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery