
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Cardiac Troponins
Related Subjects: |Cardiac Troponins |Coronary Artery AP
Cardiac troponins (cTnI and cTnT) are structural proteins within the cardiac sarcomere and the preferred biomarkers for myocardial injury. High-sensitivity assays can detect very small amounts of myocardial cell injury, but troponin ≠ myocardial infarction: MI requires a troponin rise/fall plus clinical evidence of acute myocardial ischaemia (symptoms, ECG, imaging, or coronary thrombus).
🔬 What troponin is (structure & physiology)
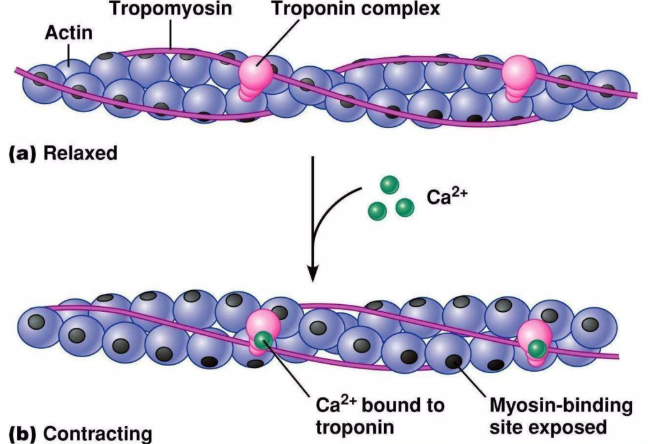
- Troponin complex sits on the thin filament (actin) with tropomyosin and regulates contraction.
- TnC binds calcium → conformational change → moves tropomyosin off actin’s myosin-binding sites → cross-bridge cycling starts.
- TnI is the inhibitory subunit (prevents actin–myosin interaction at rest).
- TnT anchors the complex to tropomyosin.
- Cardiac-specific isoforms of TnI/TnT allow blood tests to reflect cardiac myocyte injury rather than skeletal muscle damage.
🧪 High-sensitivity troponin (hs-cTn): why it changed practice
- hs-cTn assays detect low troponin concentrations with high analytical precision, enabling earlier rule-out/rule-in pathways in emergency care.
- Interpretation is assay-specific: always use your local lab’s reference ranges and pathway.
- Key concept: the clinically important threshold is the 99th percentile upper reference limit (URL) for that assay.
📌 Definitions you must get right
- Myocardial injury: any troponin value above the assay’s 99th percentile URL.
- Acute myocardial injury: myocardial injury with a rise and/or fall on serial testing (dynamic change).
- Myocardial infarction (MI): acute myocardial injury plus evidence of acute ischaemia (typical symptoms, new ischaemic ECG changes, imaging evidence, or coronary thrombus).
🩺 NICE / UK approach in practice (what you actually do in ED/AMU)
In the UK, NICE supports the use of high-sensitivity troponin testing within structured early rule-out/rule-in strategies for suspected ACS. Your hospital will implement an approved pathway (timings/cut-offs differ by assay), but the principles below stay the same.
- Always do an ECG early and treat STEMI as a time-critical emergency (troponin should not delay reperfusion).
- For possible NSTE-ACS, use hs-cTn with serial sampling when needed (especially if symptom onset is recent).
- If symptoms started very recently (e.g. within ~2 hours), a single troponin can be falsely low → repeat at an appropriate interval per local pathway.
- Discharge decisions should combine: symptoms (including ongoing pain), ECG, troponin pattern, and overall clinical risk (and safety-netting).
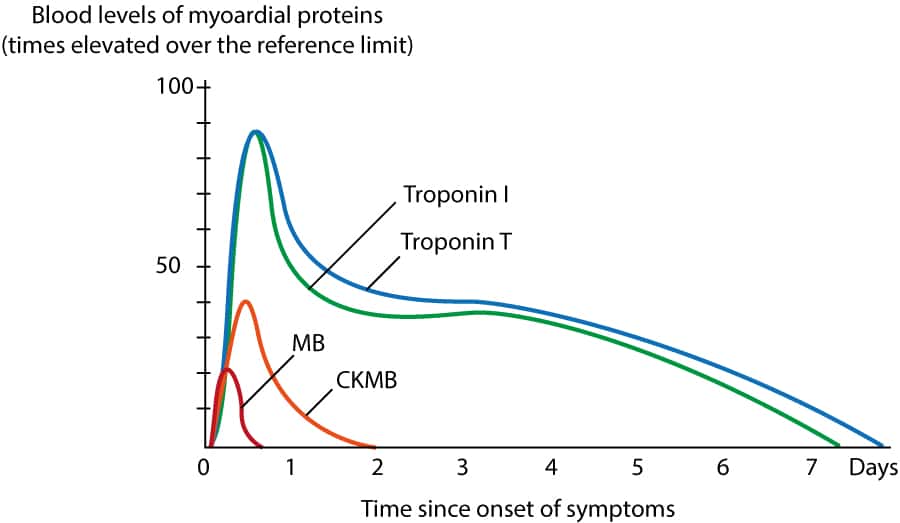
⏱️ Typical kinetics (teach the pattern, avoid overpromising)
- With contemporary assays, troponin may rise within a few hours of injury; hs-cTn can detect injury earlier than older assays.
- Early presenters can have an initially normal troponin → serial testing is essential if clinical suspicion remains.
- Troponin can remain elevated for days after significant myocardial necrosis; the exact duration varies by infarct size and assay.
🧭 How to interpret a result (a practical framework)
- Step 1 - Is it above the 99th percentile URL?
- No: MI is unlikely, but not excluded in early presenters or ongoing ischaemia → repeat if indicated.
- Yes: myocardial injury is present → move to step 2.
- Step 2 - Is there a significant rise/fall on serial testing?
- Dynamic change: suggests acute injury (consider MI vs myocarditis vs tachyarrhythmia, etc.).
- Stable elevation: suggests chronic injury (e.g. structural heart disease, CKD) - still prognostically important.
- Step 3 - Is there evidence of acute ischaemia?
- If yes → MI (type 1 or type 2 depending on mechanism).
- If no → acute myocardial injury (non-MI) and treat the cause.
⚠️ Common causes of raised troponin (MI and non-MI)
- Type 1 MI (atherothrombosis): plaque rupture/erosion → coronary thrombosis.
- Type 2 MI (supply–demand mismatch): sepsis, tachyarrhythmia, severe anaemia, hypoxia, hypertensive crisis, coronary spasm, etc.
- Acute myocardial injury (non-ischaemic): myocarditis, acute heart failure, cardiotoxic drugs, post-procedure injury, cardiac contusion.
- Chronic myocardial injury: chronic heart failure, CKD, structural heart disease - often persistently elevated with little change.
🧠 Clinical “gotchas” (very exam- and ward-relevant)
- Renal impairment: baseline troponin may be chronically elevated; the trend and clinical picture are key.
- One troponin is rarely enough if the story suggests early ACS - use serial testing as per pathway.
- Troponin is prognostic even when it’s not MI - an elevated troponin flags higher risk and warrants careful assessment.
- STEMI: treat based on ECG/clinical picture; do not wait for troponin before activating the pathway.
✅ Summary
Troponin tells you “myocardial injury happened”. To diagnose myocardial infarction you need a rise/fall above the 99th percentile URL plus evidence of acute myocardial ischaemia. In UK practice, NICE supports hs-cTn within structured early rule-out strategies - always follow your local lab’s assay-specific cut-offs and timings, and interpret results in the clinical context.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery