Related Subjects:
|Causes of abnormal Vaginal bleeding
|Vaginal Carcinoma
|Cervical cancer
|Endometrial (Uterine) Cancer
|Post Menopausal Bleeding
|AP of the Uterus and Fallopian Tubes
|AP of the Ovary
|Gynaecological History Taking
|Colposcopy
|Premature Menopause
|Polycystic Ovary syndrome
🌸 Roles
- Endocrine function: Production of steroid hormones - oestrogen, progesterone, and androgens.
- Reproductive function: Gametogenesis (development and release of oocytes).
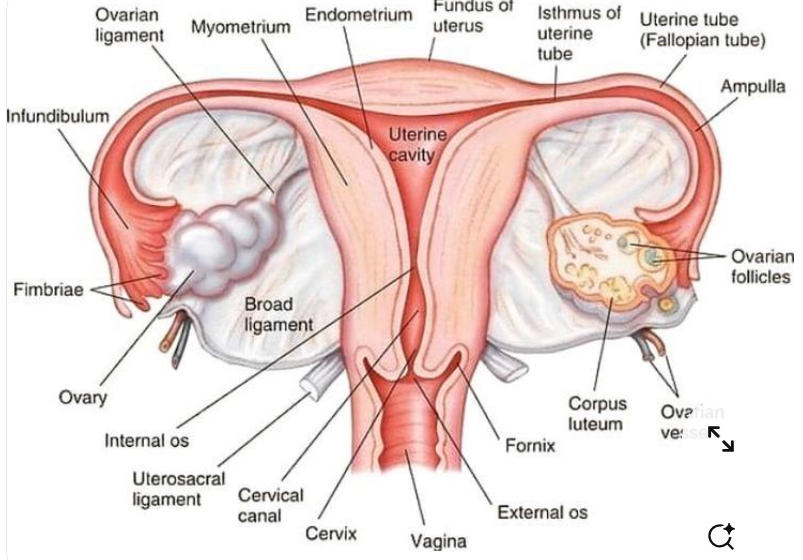
🔬 Gross Anatomy
- Paired almond-shaped organs located on either side of the uterus in the lateral pelvic wall.
- Average size in reproductive years: 4 × 3 × 2 cm; weight approximately 8–10 g.
- Lie close to the fimbrial end of the fallopian tubes, facilitating oocyte capture at ovulation.
- Attached to the posterior layer of the broad ligament by the mesovarium, a peritoneal fold carrying vessels, lymphatics, and nerves.
- Suspended laterally by the suspensory ligament of the ovary (infundibulopelvic ligament), which contains the ovarian vessels.
- Medially attached to the uterus via the ovarian ligament.
🩸 Blood Supply and Drainage
- Arterial supply: Ovarian arteries arise directly from the abdominal aorta just below the renal arteries.
- Additional contribution from the uterine artery (anastomotic supply).
- Venous drainage: Ovarian veins form the pampiniform plexus; right drains into the IVC, left drains into the left renal vein.
- Lymphatic drainage: Para-aortic (lumbar) lymph nodes.
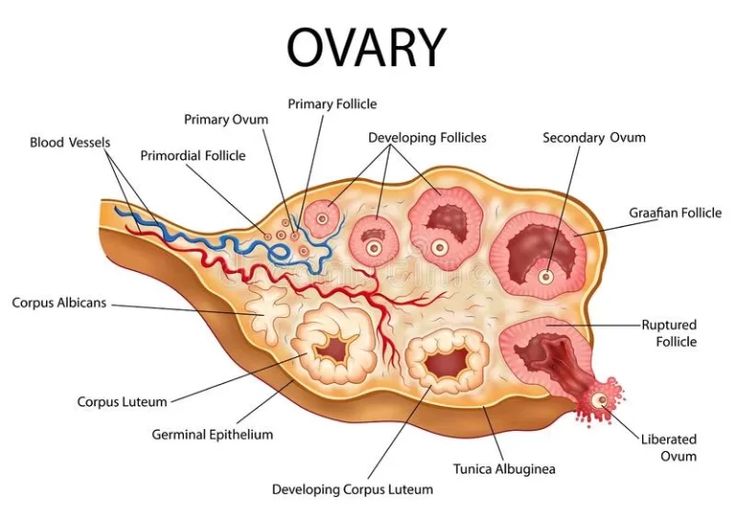
🏗️ Microscopic Structure
- Outer cortex: Contains follicles at various stages of development embedded in a dense stromal matrix.
- Inner medulla: Looser connective tissue containing blood vessels, lymphatics, and nerves.
- Surface covered by a single layer of cuboidal epithelium (historically termed “germinal epithelium”).
- Underlying dense fibrous capsule called the tunica albuginea.
- Primordial oocytes supported by stromal connective tissue and follicular cells.
🔄 Physiology: Follicular Development and Ovulation
- At menarche, approximately 400,000–500,000 primordial follicles remain in the ovarian cortex.
- Primordial follicles (~0.1 mm) consist of an oocyte surrounded by a single layer of granulosa cells.
- Granulosa cells produce oestradiol (via aromatisation of theca-derived androgens).
- Stromal cells differentiate into:
- Theca interna: Androgen-producing layer (LH-responsive).
- Theca externa: Structural layer with no endocrine function.
- During each menstrual cycle, multiple follicles are recruited under FSH influence, but usually one dominant follicle develops into a mature Graafian follicle.
- The mature follicle reaches ~20 mm in diameter before ovulation.
- The LH surge triggers completion of meiosis I:
- Primary oocyte (46 chromosomes) divides.
- Produces a secondary oocyte and first polar body (each haploid - 23 chromosomes).
- Ovulation releases the secondary oocyte into the peritoneal cavity, usually captured by the fimbriae of the fallopian tube.
🌕 Corpus Luteum Formation
- After ovulation, the ruptured follicle collapses.
- Granulosa cells become granulosa lutein cells.
- Theca interna becomes theca lutein cells.
- Forms the corpus luteum, visible as a yellow, crinkled structure.
- Secretes progesterone and oestrogen to support endometrial preparation.
- If no fertilisation:
- Degenerates after ~10–14 days.
- Forms a fibrotic scar - the corpus albicans.
- If pregnancy occurs:
- Corpus luteum enlarges (up to 3 cm).
- Persists for 8–12 weeks under hCG stimulation before placental takeover.
🥚 Oocyte Numbers Across the Lifespan
- ~7 million primordial germ cells at 15 weeks’ gestation.
- ~2 million at birth.
- ~400,000–500,000 at puberty.
- Approximately 400–500 ovulated during reproductive life.
- Remaining follicles undergo atresia.
🧠 Key Physiological Concepts
- Follicular development is regulated by the hypothalamic–pituitary–ovarian axis (GnRH → FSH/LH → ovarian hormones).
- Ovarian steroid production operates via the two-cell, two-gonadotropin model (LH stimulates theca → androgens; FSH stimulates granulosa → aromatisation to oestrogen).
- Menopause results from depletion of functional follicles, leading to reduced oestrogen and loss of negative feedback on FSH/LH.
