
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Right Ventricular ST Elevation MI (RVMI)
Related Subjects: |Atherosclerosis |Ischaemic heart disease |Assessing Chest Pain |ACS: general |ACS: NSTEMI |ACS: STEMI |ACS: Right Ventricular STEMI
❤️ Right Ventricular Myocardial Infarction (RVMI) is a specific type of STEMI affecting the RV, usually in conjunction with an inferior wall MI (both supplied by the RCA). ⚠️ Prognosis is worse due to hypotension, arrhythmias, and right-sided pump failure. The possibility of other causes (PE, pulmonary hypertension, hypovolemia) may cloud the diagnosis.
ℹ️ About
- ST-Elevation MI can involve RV ± LV.
- Associated with higher morbidity & mortality than isolated inferior MI.
🧬 Aetiology
- Isolated RV infarction (rare).
- Most commonly part of an inferior MI.
- Occlusion of the right coronary artery (RCA) → RV ischemia/infarction.
👩⚕️ Clinical Features
- Classic ACS symptoms: chest pain (± radiation), dyspnoea, nausea/vomiting.
- Triad of: • 💧 Hypotension (low preload). • ⬆️ Raised JVP (impaired RV filling). • ⛔ Clear lungs/oliguria (RV failure, not LV failure).
- Poor capillary return & signs of low cardiac output.
- May present in shock; beware confusion with PE or tamponade.
📉 ECG Lead Placement
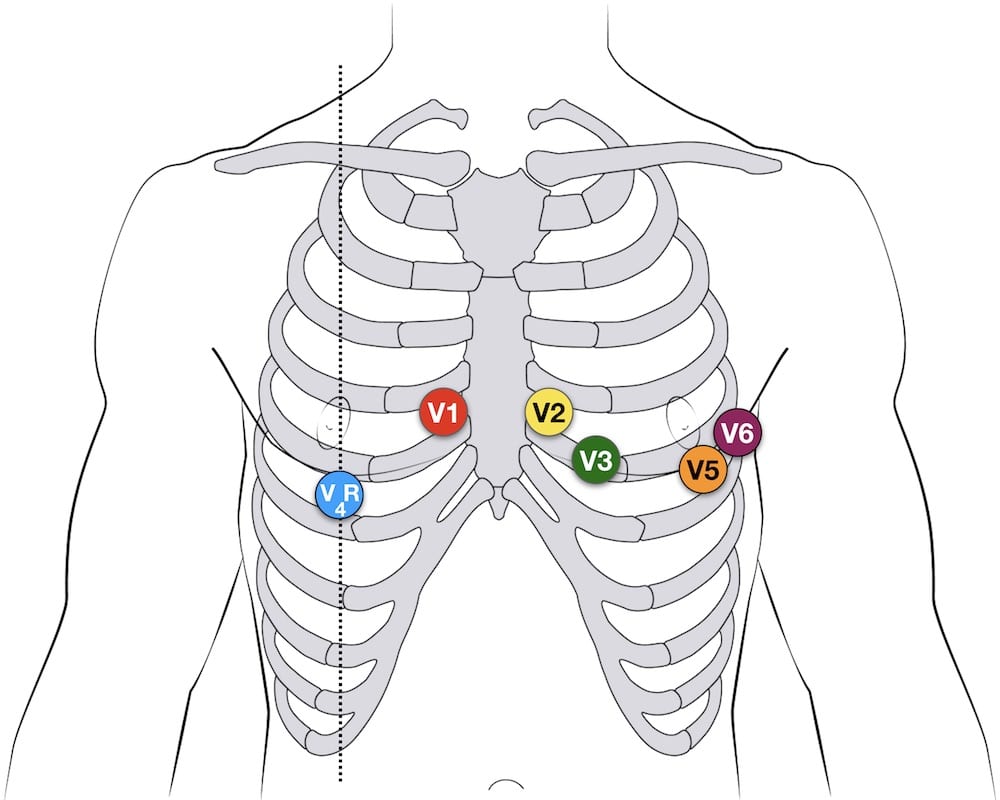
- Right-sided leads (V4R, V5R, V6R) crucial.
- ST elevation in V4R is most sensitive for RVMI. ✅
- Inferior leads (II, III, aVF) usually also show ST elevation (co-existent inferior MI).
🔎 Investigations
- 🧪 Bloods: ↑ Troponin (MI), consider D-dimer if PE suspected.
- 📉 ECG: ST elevation in right-sided leads (V4R best). Reciprocal depression in I, aVL.
- 🫀 Echo: RV wall hypokinesia, paradoxical septal motion, TR, PR, dilated IVC with poor collapse.
- 🖼️ CXR: often normal lung fields (helpful in differentiating from LV failure).
💊 Management
- ⚕️ ACS protocol: Urgent reperfusion with PCI or thrombolysis to restore RCA flow.
- 💧 Hypotension: Fluid bolus 500 mL over 15–20 min; repeat cautiously. Inotropes if unresponsive.
- 🫀 Inotropes: Dobutamine can improve RV contractility if fluids inadequate.
- ❌ Avoid nitrates & preload-reducing agents (can worsen hypotension).
- ⚠️ Watch carefully for pulmonary oedema → avoid fluid overload.
- Pain management & oxygen as per ACS guidelines.
📚 References
💡 Exam Pearl: Think RVMI in a hypotensive patient with inferior STEMI, raised JVP, clear lung fields, and ST elevation in V4R. ❌ Avoid nitrates → they reduce preload and can precipitate shock.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery