
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Ankle-Brachial Pressure Index (OSCE focused)
Related Subjects: | Vascular Surgery: Introduction | Ankle-Brachial Pressure Index (ABPI) | Peripheral Arterial Disease (PAD) | Abdominal Aortic Aneurysm (AAA) | Carotid Endarterectomy | Buerger's disease (Thromboangiitis obliterans) | Leriche syndrome (aortoiliac occlusive disease)
🦵 Ankle–Brachial Pressure Index (ABPI) - OSCE + clinic-ready
🧠 What ABPI actually measures: ABPI is a pressure ratio (ankle systolic ÷ arm systolic). In healthy arteries, ankle systolic pressure is usually similar to (or slightly higher than) brachial pressure. With a haemodynamically significant stenosis, pressure drops distal to the lesion, so the ankle pressure falls and ABPI decreases. If arteries are calcified and incompressible (e.g., diabetes/CKD), the cuff can’t occlude the vessel properly and ABPI can be falsely high - that’s when you pivot to toe pressures/toe–brachial index (TBI).
✅ When to do ABPI (high-yield indications)
- 🚶 Suspected PAD: intermittent claudication, rest pain, cold/pale foot, absent pulses.
- 🩹 Leg ulcer assessment before compression (venous vs mixed vs arterial).
- 🧦 Deciding whether compression therapy is safe and what strength to use.
- 🧠 Cardiovascular risk flag: PAD = high systemic atherosclerotic risk (think heart + brain as well as legs).
⚠️ When ABPI is unreliable / use caution
- 🪨 ABPI ≥ 1.3–1.4: suggests calcified/incompressible arteries → consider TBI, toe pressures, duplex.
- 🩸 Marked oedema, very painful wounds, severe tremor → may distort readings (technique + cuff fit matter).
- 🫀 Arrhythmias (e.g., AF) → repeat measures and average; be extra careful with technique.
- 🧠 If critical limb ischaemia/acute limb ischaemia suspected: don’t let ABPI delay urgent vascular escalation.
🧰 Equipment
- 🩺 BP cuffs (correct size!) + manual sphygmomanometer
- 📣 Handheld Doppler (commonly 5–8 MHz)
- 🧴 Gel, paper, pen (and a calm helper if you’re teaching!)
📝 Step-by-step method (Doppler ABPI)
| Step | What you do (OSCE phrasing) | Why it matters |
|---|---|---|
| 1 🛏️ Rest | Ask the patient to lie supine and rest ~10 minutes. Legs flat, not dangling. | Standardises haemodynamics (posture changes ankle pressure). |
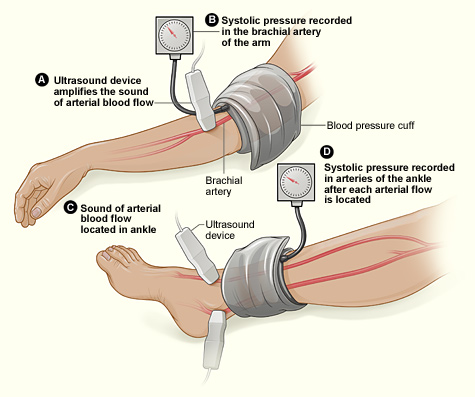
| 2 💪 Brachial pressures | Measure systolic pressure in both arms (Doppler or standard). Record both. Use the higher brachial systolic for calculations (unless subclavian stenosis suspected-see pitfalls). | Using the higher arm pressure avoids over-diagnosing PAD and improves accuracy. |
| 3 🦶 Locate ankle arteries | With Doppler + gel, find signals at dorsalis pedis and posterior tibial arteries. | You’ll measure both and use the higher ankle pressure (per leg). |
| 4 🎯 Measure ankle systolic | Place cuff just above malleoli. Inflate until Doppler signal disappears, then deflate slowly; record the pressure when signal returns = systolic. Repeat for DP and PT. | Detects the pressure distal to any stenosis; Doppler improves detection, especially in low-flow states. |
| 5 ➗ Calculate (each leg) | ABPI (Right) = highest ankle systolic (DP or PT) ÷ highest brachial systolic. Repeat for left. | This “highest ankle ÷ highest arm” method is widely recommended for accuracy. |
| 6 🧾 Document & interpret | Record: DP/PT pressures, brachials, ABPI both legs, symptoms, pulse findings, and what you’ll do next. | ABPI guides compression decisions and vascular referral urgency. |
🧮 Worked example:
Right ankle: DP 92 mmHg, PT 104 mmHg → highest ankle = 104
Brachials: R 128, L 136 mmHg → highest brachial = 136
✅ Right ABPI = 104 ÷ 136 = 0.76 → moderate PAD / mixed disease likely (compression decisions depend on ulcer context + local pathway).
📊 ABPI interpretation
| Resting ABPI | Likely interpretation | Clinical correlation |
|---|---|---|
| > 1.3 | Suggests arterial calcification / incompressible vessels | Common in diabetes, CKD, RA/vasculitis → ABPI may be unreliable |
| 0.8 – 1.3 | No evidence of significant PAD | Compression stockings generally safe (if no other contraindications) |
| 0.5 – 0.8 | Moderate PAD | Often intermittent claudication; optimise risk factors + consider imaging if severe symptoms |
| < 0.5 | Severe ischaemia | Often critical ischaemia/rest pain or tissue loss → urgent vascular input |
🧦 ABPI and compression therapy (leg ulcer context)
⚠️ Never apply compression to a new/non-healing lower leg wound until ABPI + full lower limb assessment has been done.
| ABPI | Compression guidance (typical UK community pathways) | Notes |
|---|---|---|
| 0.8–1.3 | ✅ Often suitable for full compression (if venous ulcer pattern) | Still interpret in clinical context; mixed disease can exist. |
| 0.65–0.79 | 🟠 Often reduced compression (mixed aetiology likely) | Consider tissue viability/vascular input. |
| < 0.64 | 🚫 Avoid high compression; refer per pathway | Escalate-arterial component significant. |
| < 0.5 | 🚨 Urgent vascular referral | Severe PAD likely; compression risks ischaemic injury. |
🧠 Common pitfalls (things examiners love)
- 📏 Wrong cuff size → false readings (too small cuff overestimates pressure).
- 🧍 Not resting supine → ankle pressures can be artificially high/variable.
- 💪 Only measuring one arm: you can miss a higher brachial pressure (or miss subclavian disease).
- 🪨 Falsely high ABPI in diabetes/CKD/elderly due to calcification → use TBI.
- 🚶 Symptoms with normal resting ABPI: consider exercise ABPI for claudication work-up.
🗣️ OSCE mini-script (30–45 seconds)
- 👋 “I’m going to measure the ankle–brachial pressure index to assess arterial perfusion and help guide safe management (including whether compression is appropriate).”
- 🛏️ “I’ll ask you to lie flat and rest, then measure blood pressure in both arms, then measure ankle pressures using a Doppler over dorsalis pedis and posterior tibial arteries.”
- ➗ “ABPI is the highest ankle systolic pressure divided by the highest brachial systolic pressure, calculated for each leg.”
- 🧾 “I’ll document values, interpret them with the clinical picture, and escalate urgently if severe arterial disease is suspected.”
📚 References (UK + core)
- Wounds UK / Wound Essentials: ABPI measurement and interpretation; cautions for compression; calcification/high ABPI discussion.
- Remedy BNSSG ICB: community leg ulcer assessment and ABPI thresholds guiding compression/referral.
- American Heart Association / American College of Cardiology PAD guidance: ABI <0.90 for PAD; ABI >1.40 suggests incompressible arteries; exercise ABI and TBI use.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery