Multifocal Atrial Tachycardia
Related Subjects:
|Supraventricular Tachycardia (SVT)
|Atrial Flutter
|Atrial Fibrillation
|Sinus Tachycardia
|Multifocal Atrial Tachycardia
|Junctional Tachycardia
📌 About
- Multifocal Atrial Tachycardia (MAT) is a form of supraventricular tachycardia characterised by an irregular rhythm with ≥3 distinct P wave morphologies.
- By definition, atrial rate > 100/min with variable PP, PR, and RR intervals.
- Unlike atrial fibrillation, MAT still has discrete P waves (though variable in appearance).
🧬 Aetiology & Triggers
- Multiple atrial ectopic foci firing independently.
- Usually occurs in elderly patients with underlying pulmonary disease (esp. COPD, pneumonia, PE).
- Common precipitants: hypoxia, hypercapnia, electrolyte disturbances (↓Mg, ↓K), drugs (aminophylline, theophylline, isoproterenol).
🔗 Associations
- Chronic lung disease (COPD, pulmonary hypertension).
- Ischaemic heart disease, congestive cardiac failure, diabetes.
- Post-operative states (esp. thoracic surgery).
📈 ECG Features of MAT
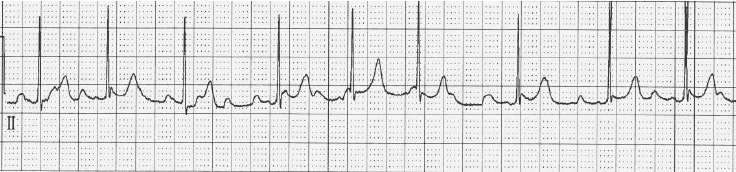
- Irregularly irregular rhythm (can mimic AF).
- ≥ 3 different P wave morphologies in the same lead.
- Atrial rate 100–180/min, with variable PR intervals.
- 1:1 conduction to the ventricles (no dropped beats as in AV block).
🩺 Clinical
- Typically in elderly patients with advanced COPD or hypoxia.
- Symptoms: palpitations, dyspnoea, sometimes chest discomfort.
- Often reasonably well tolerated; haemodynamic collapse is rare.
🔎 Investigations
- FBC: may suggest infection trigger.
- U&E: check and correct K⁺ and Mg²⁺.
- ECG: diagnostic - irregular tachycardia with ≥3 different P wave morphologies.
- CXR/ABG: assess for underlying lung pathology and hypoxia.
💊 Management
- First principles: ABC assessment.
- Treat underlying cause: optimise oxygenation, treat infection, correct electrolytes (Mg²⁺, K⁺).
- Rate control:
- Non-dihydropyridine calcium channel blockers (diltiazem, verapamil) OR beta-blockers (with caution in COPD/asthma).
- Magnesium supplementation often useful even if serum Mg normal.
- No role for: cardioversion, antiarrhythmics, or anticoagulation (unlike AF).
- Refractory cases: AV nodal ablation has been attempted, though rarely required.
📚 Key Clinical Pearls
- Differentiate from AF: MAT has visible but variable P waves, AF has none.
- Think COPD exacerbation: MAT is almost pathognomonic in elderly hypoxic COPD patients.
- Correct magnesium and potassium early: low intracellular Mg/K drives ectopy.
📖 References
