Related Subjects:
|Cardiopulmonary bypass
|Atherosclerosis
|Ischaemic heart disease
|Assessing Chest Pain
|ACS - General
|ACS - STEMI
|ACS - NSTEMI
|ACS - GRACE Score
|ACS - ECG Changes
|ACS -Cardiac Troponins
|ACS - Post MI arrhythmias
|ACS: Right Ventricular Infarction
As compared with saphenous vein grafts, radial-artery grafts for CABG show better 5-year patency (lower occlusion risk) and fewer adverse cardiac events (e.g., MI, repeat revascularisation) in RCTs and meta-analyses (NEJM 2018 RADIAL pooled analysis; HR 0.67 for composite events at 5 years). Longer-term (10-year) follow-up confirms sustained benefits in composite outcomes, though all-cause mortality difference may not always reach significance.
🫀 About CABG
- In routine clinical use since the 1960s for revascularisation in ischaemic heart disease (IHD), including stable angina, multivessel disease, and post-ACS settings.
- ~90% of patients become angina-free or significantly improved post-CABG; quality of life gains are substantial (CG126).
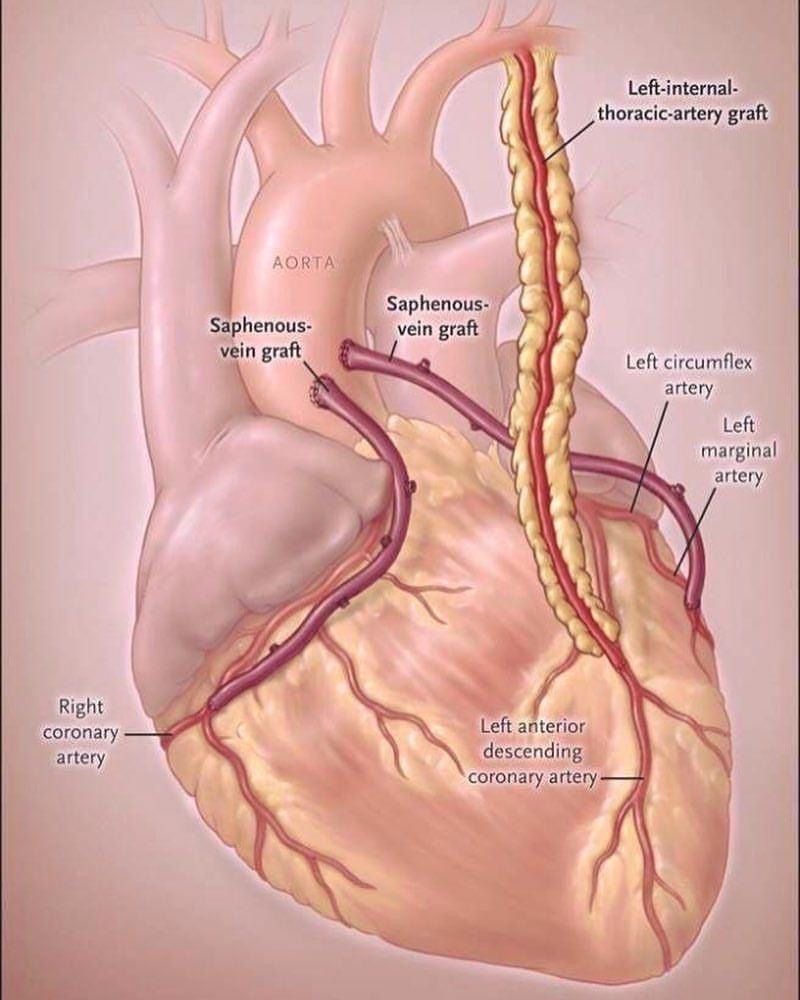
- Conduits used:
- Left Internal Mammary Artery (LIMA/ITA) to LAD – gold standard; >90–95% patency at 10–15 years due to endothelial properties and resistance to atherosclerosis.
- Saphenous vein grafts (SVG) – traditional secondary conduit; higher late failure (40–50% occlusion by 10 years due to intimal hyperplasia/atherosclerosis).
- Radial artery – increasingly used as second arterial graft; superior mid-term patency and outcomes vs SVG (5-year occlusion ~10–15% lower; better freedom from MACE in multiple trials).
- Other: Right IMA (bilateral IMA in selected low-risk patients), gastroepiploic artery (rare).
- Techniques: On-pump (cardiopulmonary bypass) standard; off-pump CABG (OPCAB) supported by NICE IPG377 (2011) for suitable patients to potentially reduce stroke risk (though large trials like CORONARY/ROOBY show similar long-term outcomes).
- Minimally invasive direct CABG (MIDCAB) or robotic-assisted options emerging in specialist centres.
- CABG provides survival benefit over medical therapy alone in:
- Left main stem (LMS) disease (>50% stenosis).
- Triple-vessel disease (TVD), especially with proximal LAD involvement or impaired LV function (ejection fraction <50%).
- Annual UK CABG volume: ~15,000–20,000 procedures; operative mortality 1–2% in elective cases (higher in emergencies/high-risk: EuroSCORE II >5%).
📌 Indications for CABG (NICE CG126 Compliant – Stable Angina Context)
- Symptoms not satisfactorily controlled despite optimal medical therapy (anti-anginals: beta-blocker/CCB first-line, add long-acting nitrate/ivabradine/nicorandil/ranolazine as needed; secondary prevention: aspirin/statins/ACEi/ARB/beta-blocker).
- Anatomical indications with survival benefit:
- Left main stem stenosis (>50%).
- Multivessel disease (proximal LAD + other vessels) where CABG offers survival advantage over PCI (SYNTAX score >22; diabetes/multivessel).
- Two-vessel disease including proximal LAD.
- Complex anatomy unsuitable for PCI (e.g., chronic total occlusions, diffuse disease).
- Moderately impaired LV function (EF 30–50%) with viable myocardium – CABG improves outcomes vs medical therapy.
- Post-ACS revascularisation (NG185): Consider CABG if anatomy suitable and patient stable (e.g., incomplete revascularisation by PCI, LMS involvement).
- Heart team discussion mandatory (cardiologist + surgeon) for complex cases (CG126 1.5).
⚠️ Complications (Peri- & Post-Operative)
- Sternal wound infection/mediastinitis (1–3%; higher in diabetes/obesity; deep sternal wound ~0.5–1%).
- Atrial fibrillation (new-onset in 20–40%; peaks day 2–4; usually self-limiting but increases stroke risk).
- Stroke (1–2%; higher in aortic atheroma, off-pump may reduce in some subgroups).
- Graft failure/occlusion (SVG > arterial; early technical, late atherosclerotic).
- Perioperative MI, low cardiac output syndrome.
- Renal dysfunction (AKI in 5–20%; dialysis ~1–2%).
- Pulmonary complications (atelectasis, pneumonia).
- GI (mesenteric ischaemia rare but serious), neurological (delirium), bleeding/tamponade.
- Long-term: progressive native vessel/ graft disease; leg wound issues from SVG harvest.
💊 Peri-Operative Management & Issues
- Antiplatelets: Continue aspirin lifelong; stop P2Y12 inhibitors (clopidogrel 5 days, ticagrelor 5–7 days, prasugrel 7 days) pre-op unless high-risk ACS.
- Anticoagulation: Heparin during CPB (ACT-guided); protamine reversal.
- Antibiotic prophylaxis: Broad-spectrum (e.g., cefuroxime) to prevent surgical site infection.
- Operative mortality: 1–2% elective (EuroSCORE II); higher in octogenarians/emergencies (3–10%).
- Enhanced recovery after surgery (ERAS) protocols: Early mobilisation, multimodal analgesia, minimised drains, goal-directed fluid therapy – reduce length of stay to 5–7 days.
📈 Long-Term Outcomes & Secondary Prevention
- Arterial grafts (LIMA > radial) superior patency: LIMA ~90% at 10–15 years; radial ~80–90% at 5–10 years vs SVG ~50–60% at 10 years.
- Survival benefit: Proven in LMS/TVD vs medical therapy; CABG + optimal medical therapy reduces MACE vs PCI in complex disease (FREEDOM trial in diabetes).
- Radial vs SVG: Lower adverse events at 5–10 years (death/MI/revascularisation); women may derive greater benefit.
- Repeat revascularisation: Often via PCI to native vessels or grafts.
- Secondary prevention essential: Aspirin (or clopidogrel if intolerant), high-intensity statin, ACEi/ARB, beta-blocker (if LV dysfunction), smoking cessation, cardiac rehabilitation (improves adherence/outcomes).
- Quality of life: Dramatic improvement; most return to normal activities within 3–6 months.
📚 References (Current as of March 2026)
