Related Subjects:
|Status Epilepticus (Epilepsy)
|Coma management
|Lorazepam
|Phenytoin
|Levetiracetam
|Epilepsy - General Management
|First Seizure
|Epilepsy in Pregnancy
|Febrile seizures
⚡ Idiopathic Generalised Epilepsy (IGE) is a group of epilepsy syndromes characterised by generalised seizures, normal neuroimaging, and a presumed genetic basis.
It accounts for ~15–20% of all epilepsies and typically presents in childhood or adolescence.
🔎 About
- IGE is also called “genetic generalised epilepsy” (GGE) in newer classifications.
- Onset is usually in childhood or adolescence, often between ages 5–20.
- Patients have normal neurological examination and normal neuroimaging.
- There is often a family history of seizures or epilepsy.
🧬 Pathophysiology
- Thought to result from genetic predisposition affecting neuronal excitability and cortical network synchronisation.
- Involves abnormal thalamocortical oscillations → generalised 3 Hz spike-and-wave discharges.
- No structural brain abnormality on MRI (distinguishes it from focal epilepsies).
🩺 Clinical Syndromes under IGE
- Childhood Absence Epilepsy (CAE)
– Onset: 4–10 years.
– Frequent absence (“blank”) seizures, often unnoticed at first.
– EEG: 3 Hz spike-and-wave discharges.
- Juvenile Absence Epilepsy (JAE)
– Onset: 10–16 years.
– Absences less frequent than CAE, but generalised tonic–clonic seizures common.
- Juvenile Myoclonic Epilepsy (JME)
– Onset: adolescence (12–18 years).
– Myoclonic jerks in the morning (“I keep dropping things at breakfast ☕”).
– Often associated with tonic–clonic seizures.
- Generalised Tonic–Clonic Seizures Alone (GTCSa)
– Onset: adolescence.
– No absences/myoclonus, just generalised tonic–clonic seizures.
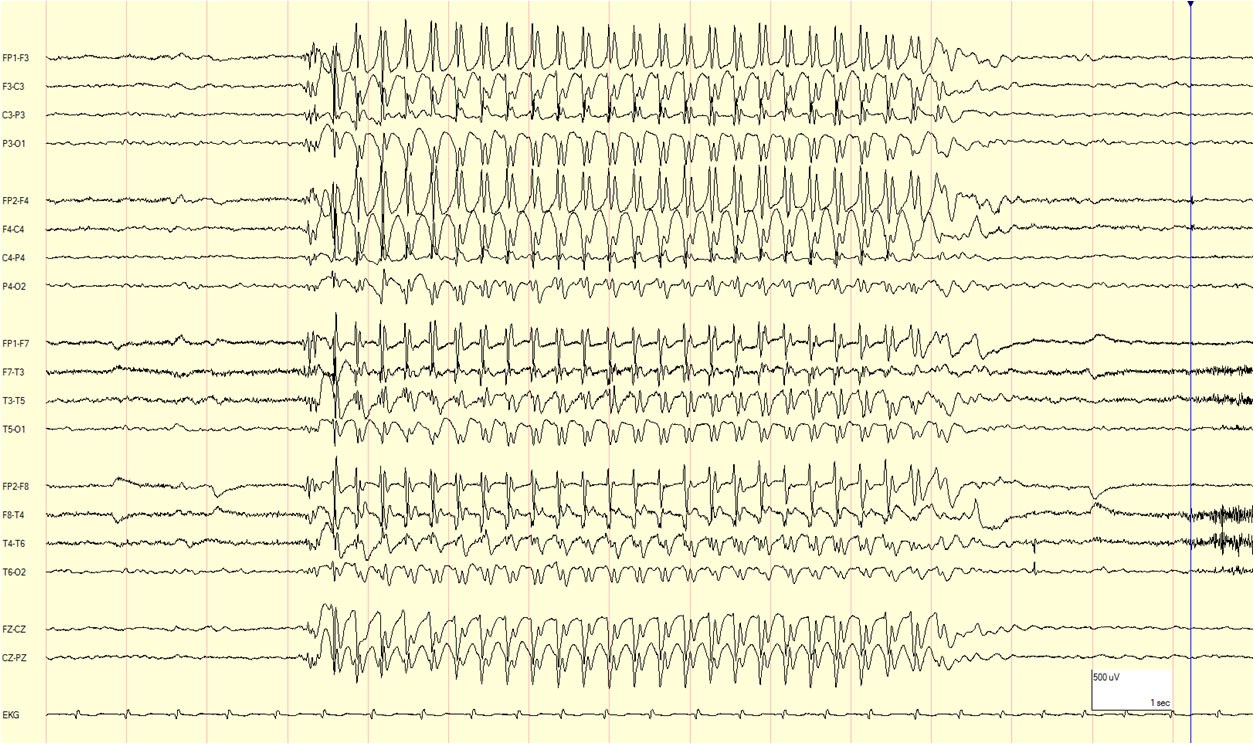
Example of 3Hz generalized spike-wave seen on the ictal EEG
📊 Risk Factors / Triggers
- Sleep deprivation 🛌.
- Alcohol, especially binge drinking 🍺.
- Photosensitivity (flashing lights, screens) 💡.
- Stress, illness, hormonal changes.
🧪 Investigations
- EEG: hallmark = generalised 3 Hz spike-and-wave (absences) or polyspike-and-wave (JME).
- Neuroimaging (MRI): Normal – helps exclude structural causes.
- Bloods: To rule out metabolic triggers (glucose, electrolytes, calcium, magnesium).
- History: Careful witness account; absence seizures often misdiagnosed as daydreaming.
💊 Management
- First-line AEDs:
– Sodium valproate (⚠️ avoid in women of childbearing age due to teratogenicity, neurodevelopmental risk).
– Alternatives: Levetiracetam, Lamotrigine (slightly less effective in JME but safer in women).
- Lifestyle: Sleep hygiene, avoid alcohol binges, stress management, photosensitivity precautions.
- Driving: Must be seizure-free for at least 12 months before driving (DVLA rules, UK).
- Counselling: Important to explain precipitating factors and need for adherence.
⚠️ Drugs to Avoid
- Carbamazepine and phenytoin may worsen generalised seizures in IGE.
- Gabapentin and tiagabine are not effective.
📚 Prognosis
- Generally good with treatment – many achieve remission, though some require lifelong AEDs.
- Absence epilepsy often resolves by adolescence.
- Juvenile myoclonic epilepsy tends to persist into adulthood (lifelong tendency).
📌 Exam Pearls
- IGE = normal neuro exam + normal MRI + abnormal EEG (generalised discharges).
- Morning myoclonus in a teenager = Juvenile Myoclonic Epilepsy.
- Child who “daydreams” with 3 Hz spike-wave = Childhood Absence Epilepsy.
- Avoid carbamazepine → may exacerbate seizures.
- Valproate most effective, but avoid in women of childbearing age 🚫🤰.
