
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Subdural haematoma
Related Subjects: |Brain Herniation syndromes |Epidural Haematoma |Subdural haematoma |Extradural haematoma🩸 A Subdural Haematoma (SDH) is bleeding into the potential space between the dura mater and arachnoid mater. 🧠 Classically venous in origin (torn bridging veins), producing a slower and often insidious presentation compared with extradural haematoma. ⚠️ Always suspect SDH in elderly, alcohol-dependent, anticoagulated, or cognitively declining patients after even minor trauma.
💡 Pathophysiology (What is really happening)
- Acceleration–deceleration forces tear bridging veins traversing from cortex to dural sinuses.
- Venous pressure is low → gradual accumulation → delayed neurological decline ⏳.
- Cerebral atrophy (ageing, alcohol misuse) increases vein length and fragility.
- In chronic SDH, inflammatory membranes form and become vascularised (often via middle meningeal artery branches), predisposing to recurrence.
- Mass effect → midline shift → raised intracranial pressure (ICP) and risk of herniation.
🧬 Classification by Time Course
- Acute: <72 hours (hyperdense on CT).
- Subacute: 3–21 days (may appear isodense).
- Chronic: >3 weeks (hypodense; liquefied).
📌 Risk Factors
- Falls (especially >65 years) 👴
- Alcohol misuse 🍺
- Anticoagulants (warfarin, DOACs) and antiplatelets 💊
- Coagulopathy or thrombocytopenia
- Low CSF pressure (post-LP, VP shunt)
- Epilepsy or high-impact trauma 🚗
🩺 Clinical Features
Presentation varies with bleed rate and cerebral reserve. Acute SDH often mimics severe TBI; chronic SDH frequently masquerades as delirium or dementia.
- Acute: ↓ GCS, severe headache 🤕, vomiting, seizures, focal deficit.
- Chronic: Progressive confusion, personality change, gait disturbance, falls.
- Focal signs: hemiparesis, aphasia, visual field deficit.
- Unilateral dilated pupil (CN III compression) → impending herniation 🚨.
- Cushing response: bradycardia + hypertension + irregular breathing.
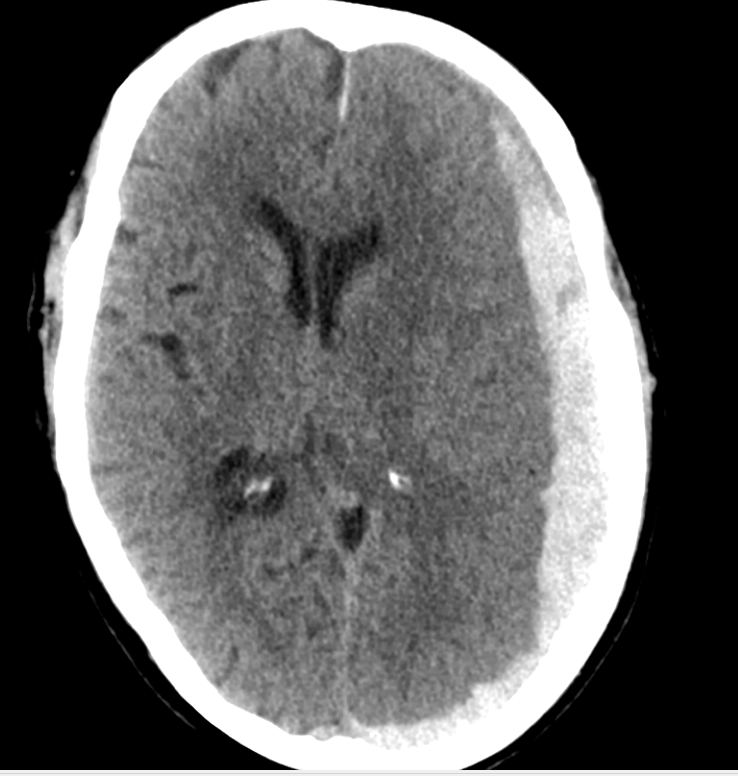
📷 Imaging
CT Head (First-line)
- Crescent-shaped extra-axial collection.
- Crosses suture lines but limited by dural reflections (falx, tentorium).
- Assess thickness, midline shift, basal cistern effacement.
Large Subacute SDH with Midline Shift

Large Acute SDH
MRI is helpful when CT is equivocal (isodense collections, posterior fossa, chronic cases).
🔬 Investigations
- Bloods: FBC, U&E, clotting screen, group & save.
- Urgently check INR if on warfarin.
- Platelets ideally >100 × 10⁹/L for surgery.
- CT cervical spine in trauma.
⚠️ Complications
- Raised ICP and transtentorial herniation 🧠
- Recurrent chronic SDH (10–20%)
- Seizures
- Infarction from vascular compression
- Subdural empyema (rare)
⚡ Management
All moderate or large SDHs require early neurosurgical discussion. Management is guided by neurological status and imaging findings.
- Initial (ABC): Airway protection if GCS ≤8; maintain normoxia and normocapnia.
- Reverse anticoagulation:
- Warfarin → IV vitamin K + PCC.
- DOAC → specific reversal agents if available.
- Surgical Indications:
- Thickness >10 mm OR midline shift >5 mm.
- Neurological deterioration.
- Acute SDH: Craniotomy ± decompressive craniectomy.
- Chronic SDH: Burr-hole drainage ± subdural drain.
- Conservative: Small, asymptomatic SDH with close observation and repeat imaging 👀.
- Consider MMA embolization in recurrent chronic SDH.
🆘 Red Flags (Call Neurosurgery Immediately)
- Deteriorating GCS
- New pupillary asymmetry
- Progressive focal deficit
- Significant midline shift on imaging
📋 EDH vs SDH Comparison
🟥 EDH: Arterial (middle meningeal), biconvex, does NOT cross sutures, lucid interval possible.
🟦 SDH: Venous, crescent-shaped, CAN cross sutures, often delayed presentation.
⚠️ Confusion + fall + anticoagulation = SDH until proven otherwise.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery