
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Glioblastoma ✅
Related Subjects: |Brain tumours |Astrocytomas |Brain Metastases |Tuberous sclerosis |Turcot's syndrome |Lhermitte Duclos Disease |Oligodendroglioma |Acute Hydrocephalus |Intracranial Hypertension |Primary CNS Lymphoma (PCNSL) |Astrocytomas |Glioblastoma
🧠 Glioblastoma (GBM) is the most aggressive primary malignant brain tumour in adults and is classified as a WHO Grade 4, IDH-wildtype diffuse astrocytic tumour. It is characterised by ⚡ rapid growth, 🕸️ diffuse infiltration, and 💊 relative resistance to therapy. In UK practice, it is managed via a specialist neuro-oncology MDT, with treatment aimed at prolonging survival and maintaining quality of life rather than cure. Crucially, GBM behaves as a diffuse infiltrative disease, explaining why recurrence is inevitable despite optimal treatment.
📊 Epidemiology
- 📈 Most common malignant primary brain tumour in adults.
- 👴 Peak age: 6th–7th decade.
- ♂️ Slight male predominance.
- 👶 Rare in children (different molecular subtypes).
- 🌍 UK incidence ~3–4 per 100,000/year.
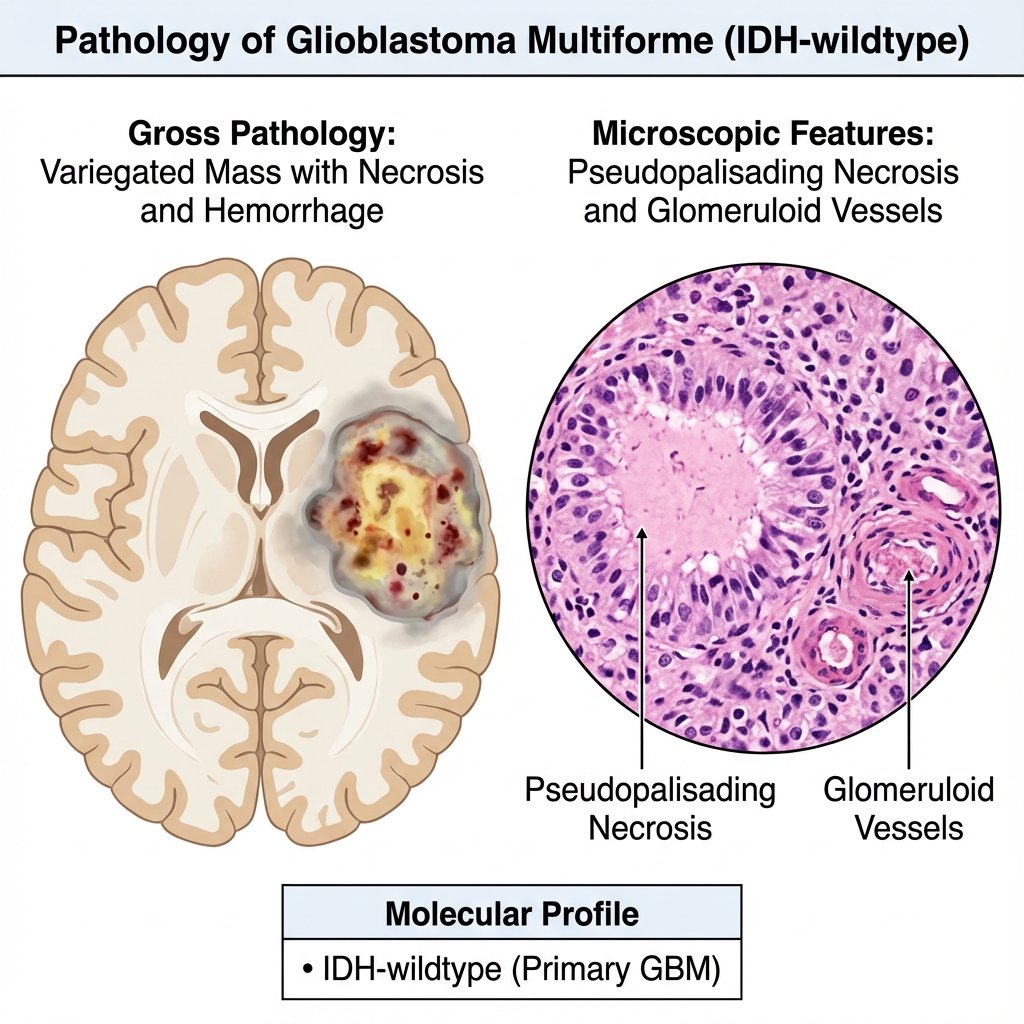
🧬 Pathophysiology
GBM arises from astrocytic lineage cells that acquire multiple oncogenic mutations. Its hallmark is 🕸️ diffuse invasion along white matter tracts, meaning complete resection is impossible. Hypoxia within the tumour drives 🔥 VEGF-mediated angiogenesis, resulting in abnormal vessels, oedema, and contrast enhancement on imaging. From a clinical reasoning perspective, mass effect + infiltration + oedema together explain symptoms and radiological findings.
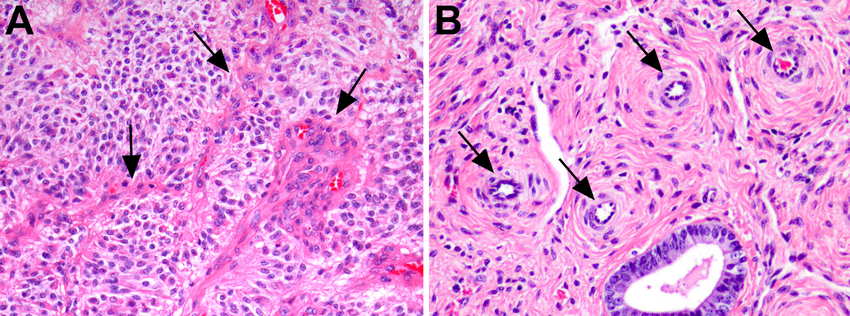
- ☠️ Pseudopalisading necrosis → reflects tumour hypoxia (classic histology).
- 🩸 Microvascular proliferation → leaky vessels causing vasogenic oedema.
- 🕷️ Diffuse infiltration → recurrence even after “complete” resection.
🧬 Molecular Classification (WHO 2021)
WHO classification now prioritises molecular features over histology. Adult GBM is defined as an IDH-wildtype diffuse astrocytic tumour with characteristic molecular abnormalities, even if histology is not classic. This aligns with modern UK neuro-oncology pathways and clinical trial stratification.
- 🧬 IDH-wildtype (defining feature).
- 🧬 TERT promoter mutation.
- 📡 EGFR amplification.
- 🧾 Chromosome +7 / −10 signature.
- 💊 MGMT promoter methylation → predicts better response to temozolomide.
🩺 Clinical Features
Symptoms typically evolve over weeks to months, helping distinguish GBM from lower-grade gliomas. Features reflect raised intracranial pressure, focal neurological dysfunction, and cortical irritation. New-onset seizures in an adult should always prompt consideration of an underlying brain tumour.
- 🤕 Progressive headache (often worse in morning).
- ⚡ New-onset seizures.
- 🦾 Focal deficits (e.g. weakness, aphasia, visual field loss).
- 🧠 Cognitive or personality change (frontal lobe involvement).
- 🤢 Nausea/vomiting (raised ICP).
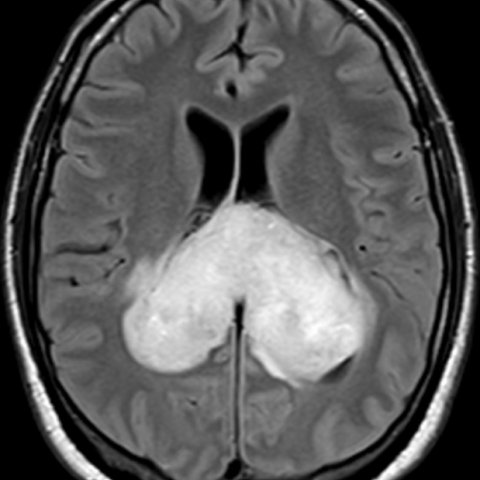
🧠 Neuroimaging
MRI brain with contrast is the investigation of choice in NICE pathways. Imaging reflects necrosis, angiogenesis, and vasogenic oedema. Always consider differentials such as metastasis or abscess in ring-enhancing lesions.
- 🌀 Irregular ring-enhancing lesion on T1 post-contrast.
- ⚫ Central necrosis.
- 🌊 Extensive surrounding T2/FLAIR oedema.
- 📊 Increased perfusion (tumour vascularity).
🧪 Diagnosis
Definitive diagnosis requires histological and molecular confirmation. NICE-aligned care emphasises obtaining tissue safely while minimising neurological deficit. Management decisions are made in a neuro-oncology MDT.
- 🔪 Maximal safe surgical resection (preferred).
- 🎯 Stereotactic biopsy if unresectable or deep lesion.
- 🧬 Mandatory molecular profiling.
🦋 Butterfly GBM
Tumours crossing the corpus callosum create a “butterfly” appearance on MRI. This indicates highly infiltrative disease and is associated with poorer prognosis.
💊 Management (NICE-aligned)
Treatment is multimodal and palliative, focusing on prolonging survival and preserving function. Standard of care in fit patients is the Stupp protocol.
- 🔪 Maximal safe resection.
- 📡 Radiotherapy (typically 60 Gy in 30 fractions).
- 💊 Temozolomide (concurrent + adjuvant).
- 💉 Dexamethasone for cerebral oedema (shortest duration possible).
- 💊 Antiepileptics only if seizures occur (not prophylactic per NICE).
- 🤝 Early palliative care involvement.
📉 Prognosis
GBM carries a poor prognosis due to its infiltrative nature and resistance to therapy. Outcomes depend heavily on performance status, extent of resection, and molecular profile. MGMT methylation improves response to chemotherapy, highlighting the importance of molecular testing.
- ⏳ Median survival: ~12–18 months.
- 📉 Worse with older age and poor functional status.
- 💊 Better response with MGMT promoter methylation.
🎯 Key Learning Points
- 🧬 GBM is defined by IDH-wildtype molecular status.
- 🕸️ Diffuse infiltration explains inevitable recurrence.
- 💊 Standard treatment = surgery + radiotherapy + temozolomide.
- 🚫 Do not give prophylactic antiepileptics (NICE).
- 🤝 Early honest prognostic discussions are essential in UK care.
📚 References (NICE, UK & International Guidance)
-
🇬🇧 NICE Guideline NG99: Brain tumours (primary) and brain metastases in adults
🔗 https://www.nice.org.uk/guidance/ng99
Core UK guidance on diagnosis, imaging, MDT management, surgery, radiotherapy, chemotherapy, and palliative care. -
🚨 NICE Guideline NG12: Suspected cancer: recognition and referral
🔗 https://www.nice.org.uk/guidance/ng12
Primary care referral thresholds and red flag symptoms for brain tumours. -
🏥 NHS England: Neuro-oncology Service Specification
🔗 NHS England Neurosciences Service Specification
Defines MDT care, specialist centres, and UK service delivery standards. -
🧠 EANO Guidelines (2021/2023): Diffuse Gliomas in Adults
European gold-standard guidance on molecular classification, treatment pathways, and recurrence management. -
🌍 WHO Classification of CNS Tumours (5th Edition, 2021)
Defines glioblastoma as an IDH-wildtype diffuse astrocytic tumour with molecular criteria. -
📖 Stupp R et al. (2005): Radiotherapy plus Concomitant and Adjuvant Temozolomide
🔗 NEJM Landmark Trial
Established the current standard of care (Stupp protocol). -
📘 Oxford Handbook of Clinical Medicine
Concise UK-focused overview of brain tumours and clinical presentation. -
📗 Kumar, Abbas & Aster – Robbins & Cotran Pathologic Basis of Disease
Detailed explanation of GBM histology and pathophysiology (pseudopalisading necrosis, angiogenesis). -
📙 Davidson’s Principles and Practice of Medicine
UK core textbook covering clinical features, diagnosis, and management of brain tumours. -
🧪 UpToDate: Glioblastoma in adults
Comprehensive, regularly updated clinical review (useful for deeper learning and nuance). -
🧬 cIMPACT-NOW Updates
Refinements to WHO molecular classification of gliomas.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery