Related Subjects:
|Adrenaline/Epinephrine
|Atropine
|Adult Resus:Acute Anaphylaxis
|Adult Resus:Basic Life Support
|Adult Resus: Advanced Life Support
|Adult Resus: Obstetric Cardiac Arrest
|Newborn/Child Resus: All
|Acute Hypotension
|Cardiogenic shock
|Distributive Shock
|Hypovolaemic or Haemorrhagic Shock
|Obstructive Shock
|Septic Shock and Sepsis
|Shock (General Assessment)
|Toxic Shock Syndrome
|Resus:Bradycardia
|Resus:Tachycardia
|Resus:Hyperkalaemia
|Resus:Post Resuscitation Algorithm
|Resus:Acute Severe Asthma
|Resus:Acute Haemorrhage
🚨 Collapsed & Unresponsive Adult
➡️ Check safety ⚠️ → Check response 📢 → Call for help / activate emergency response 📞
➡️ Open airway 🤲 → Check breathing for no more than 10 seconds
➡️ Not breathing normally? Call 999 / arrest team and start CPR immediately ❤️🔥
➡️ CPR: 30 compressions : 2 breaths if trained and able
➡️ Send for AED / defibrillator and attach as soon as available ⚡
🔄 Basic Life Support (BLS) Overview
- BLS aims to maintain cerebral and coronary perfusion until defibrillation and definitive care are available.
- Early recognition, early CPR and early defibrillation are major predictors of survival.
- Agonal gasps, occasional gasping, seizure-like movements or very abnormal breathing should be treated as not breathing normally.
- Do not wait for senior review before starting CPR.
- If the patient is unresponsive but breathing normally, place in the recovery position, call for help and monitor closely.
🚦 Arrest or Deteriorating Patient?
| Situation |
Immediate approach |
| Unresponsive and not breathing normally |
Cardiac arrest pathway: call for help, start CPR, attach AED/defib, follow prompts. |
| Unresponsive but breathing normally |
Recovery position, call for help, monitor breathing, reassess frequently. |
| Deteriorating patient with signs of life |
Use ABCDE assessment and treat problems as they are found. |
| After ROSC |
ABCDE reassessment, oxygenation/ventilation, ECG, BP support, glucose, temperature and senior/ICU review. |
🩺 Primary Survey: ABCDE Approach
Use ABCDE for the acutely unwell patient who has signs of life, or after return of spontaneous circulation.
In confirmed cardiac arrest, start CPR and defibrillation rather than delaying for a full ABCDE assessment.
| Component |
Assessment |
Immediate Action |
| 🛫 Airway |
Patency, obstruction, secretions, vomit, blood, foreign body |
Open airway, suction, remove visible obstruction, airway adjuncts if trained |
| 🫁 Breathing |
Rate, effort, oxygen saturations, chest symmetry, breath sounds |
Oxygen if hypoxic, assist ventilation if inadequate, treat reversible causes |
| ❤️ Circulation |
Pulse, BP, capillary refill, skin temperature, bleeding, ECG rhythm |
IV access, fluids/blood if indicated, treat shock, CPR if no signs of circulation |
| 🧠 Disability |
AVPU/GCS, pupils, glucose, seizures, drugs/toxins |
Treat hypoglycaemia, control seizures, consider naloxone if opioid toxicity suspected |
| 🧍 Exposure |
Temperature, rash, trauma, bleeding, devices, full examination |
Look for clues, treat sepsis/anaphylaxis/trauma, prevent hypothermia |
👀 Initial Recognition and Safety
- ⚠️ Ensure scene safety: traffic, electricity, water, chemicals, violence, sharps.
- 🤝 Shake shoulders gently and shout: “Are you alright?”
- 👁️ Look for purposeful movement, normal breathing or speech.
- ❌ No response = medical emergency.
- 📞 Activate emergency response early: 999 in the community or arrest team in hospital.
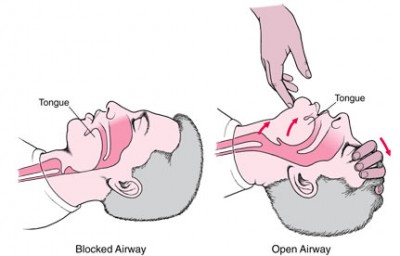
🛫 Airway: Assessment and Management
Loss of airway tone is common in unconscious patients. Tongue obstruction, secretions, vomit, blood or foreign material may obstruct the airway.
- 🤲 Perform head-tilt / chin-lift unless cervical spine injury is suspected.
- 📢 Use jaw thrust if cervical spine injury is suspected.
- 🦷 Remove only visible foreign bodies, vomit or loose dentures.
- 🪥 Leave well-fitting dentures in place unless loose or obstructing.
- 🧪 Insert an oropharyngeal or nasopharyngeal airway if trained and appropriate.
- 📞 Escalate early if airway obstruction persists or GCS is low.
| 🚫 Signs of Airway Obstruction |
🩺 Immediate Management |
- Snoring, gurgling or stridor
- Choking or inability to speak
- Paradoxical chest/abdominal movement
- Central cyanosis
- Falling oxygen saturations
- Reduced consciousness
|
- Airway manoeuvres
- Suction if available
- Remove visible obstruction
- Airway adjuncts if trained
- High-flow oxygen if breathing but hypoxic
- Bag-valve-mask ventilation if inadequate breathing
- Adrenaline IM if anaphylaxis suspected
- Prepare for advanced airway support
|
🫁 Breathing: Assessment and Support
Check breathing by looking, listening and feeling for normal breathing for no more than 10 seconds.
Agonal gasps are not normal breathing and should trigger CPR.
- 👁️ Look: chest movement, respiratory effort, symmetry, cyanosis.
- 👂 Listen: breath sounds, stridor, wheeze, gurgling.
- 🤚 Feel: airflow at the mouth/nose.
- ⏱️ Assess breathing for ≤10 seconds.
- ⚠️ Agonal gasps, occasional gasping or abnormal breathing = treat as cardiac arrest.
- 💨 Give oxygen if hypoxic or critically unwell and trained to do so.
- 🫁 Assist ventilation with bag-valve-mask if breathing is inadequate.
- 📞 Call for senior / anaesthetic / ICU support early if ventilation is failing.
| Common Causes of Acute Breathlessness / Respiratory Collapse |
- Pulmonary oedema
- Pulmonary embolism
- Pneumonia or sepsis
- Pneumothorax, including tension pneumothorax
- Asthma or COPD exacerbation
- Anaphylaxis
- DKA or severe metabolic acidosis
- Opioid or sedative toxicity
|
❤️ Circulation: Perfusion and CPR
Loss of effective circulation leads to rapid cerebral hypoxia. High-quality chest compressions maintain some coronary and cerebral perfusion until defibrillation and advanced care are available.
- Healthcare professionals may check carotid or femoral pulse, but do not spend more than 10 seconds.
- If there are no signs of life, no normal breathing, or doubt about the presence of a pulse, start CPR.
- Do not delay CPR for prolonged pulse checks.
❤️🔥 High-Quality Chest Compressions
- Hands in the centre of the chest, on the lower half of the sternum.
- Compression depth: 5–6 cm.
- Compression rate: 100–120/min.
- Allow full chest recoil.
- Minimise interruptions.
- Change compressor about every 2 minutes if possible to prevent fatigue.
💋 Rescue Breaths: 30:2
- Open airway.
- Pinch nose.
- Seal mouth over the patient’s mouth.
- Give each breath over about 1 second.
- Look for visible chest rise.
- Give two effective breaths, then restart compressions immediately.
✋ Compression-Only CPR
If untrained, unable or unwilling to give rescue breaths:
- Give continuous chest compressions.
- Rate 100–120/min.
- Minimise pauses.
- Use speakerphone so the emergency call handler can guide CPR.
| ⚡ AED / Defibrillator |
Action |
| Send for AED/defib early |
Do not leave the patient if alone unless necessary; ask someone else to fetch it. |
| Attach pads |
Expose chest, attach pads firmly, follow AED/defib prompts. |
| During analysis/shock |
Ensure nobody is touching the patient. |
| After shock or no shock advised |
Restart CPR immediately unless there are clear signs of life. |
| 🩸 Causes of Circulatory Collapse / Arrest |
- Acute coronary syndrome / malignant arrhythmia
- Massive pulmonary embolism
- Major haemorrhage
- Sepsis
- Anaphylaxis
- Cardiogenic shock
- Cardiac tamponade
- Tension pneumothorax
- Severe hypoxia
- Severe electrolyte disturbance, especially hyperkalaemia
|
🧠 Disability: Neurological Status
- A – Alert
- V – Responds to Voice
- P – Responds to Pain
- U – Unresponsive
🧪 Check capillary glucose early.
💉 Treat hypoglycaemia immediately.
💊 Consider opioid overdose → naloxone if appropriate.
🫁 Low GCS or loss of airway reflexes = airway risk → urgent anaesthetic / senior review.
🧠 Consider CT head once stabilised if neurological cause, trauma or anticoagulation is suspected.
🧍 Exposure: Full Assessment
- Undress respectfully and preserve dignity.
- Inspect for trauma, bleeding, rash, medical alert jewellery, needle marks or signs of sepsis.
- Check drains, catheters, cannulas, medication patches and infusion pumps.
- Measure temperature.
- Prevent hypothermia and re-cover the patient promptly.
🔁 Reversible Causes of Cardiac Arrest: 4 Hs and 4 Ts
| 4 Hs |
4 Ts |
- Hypoxia
- Hypovolaemia
- Hypo-/hyperkalaemia and metabolic disturbance
- Hypothermia
|
- Thrombosis — coronary or pulmonary
- Tension pneumothorax
- Tamponade
- Toxins
|
📌 Key Learning Points
- Unresponsive + not breathing normally = cardiac arrest until proven otherwise.
- Agonal gasps are not normal breathing.
- Start CPR immediately; do not wait for a doctor, monitor or ECG.
- High-quality compressions and early defibrillation save lives.
- Use ABCDE for patients with signs of life, peri-arrest patients, and after ROSC.
📸 Practical Illustrations

📚 References
- Resuscitation Council UK: Adult Basic Life Support Guidelines, 2025.
- Resuscitation Council UK: Executive summary of main changes since 2021 guidelines, 2025.
- NICE CKS: Cardiac arrest — out-of-hospital care: Basic life support adult.
```
