
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Haematuria
Related Subjects: Acute Kidney Injury
🚑 Initial Emergency Management of Severe Haematuria
| Step | Action | Key Notes |
|---|---|---|
| 1️⃣ Resuscitation | Assess ABC: oxygen, IV access, monitoring, fluid resuscitation if hypotensive. | Heavy haematuria can cause hypovolaemia & shock. |
| 2️⃣ Investigations at Presentation | FBC, U&E, clotting, G&S / cross-match; urine dip & MSSU. | Check Hb for anaemia, INR if anticoagulated. |
| 3️⃣ Bladder Drainage | Insert large-bore 3-way Foley catheter (22–24Fr). Irrigate manually until clear → start continuous bladder irrigation. | Avoid catheter if urethral injury suspected (e.g. pelvic fracture, blood at meatus). |
| 4️⃣ Analgesia | Give strong analgesia as required (often colicky pain with clots). | Opioids may be required for severe discomfort. |
| 5️⃣ Correct Reversible Causes | Reverse anticoagulation if excessive; treat infection if septic. | Discuss with haematology if complex anticoagulant reversal needed. |
| 6️⃣ Urology Referral | Urgent referral if clot retention, persistent bleeding, solitary kidney, obstruction, or haemodynamic compromise. | All macroscopic haematuria should have urology follow-up (cystoscopy + imaging). |
🚨 The key concern in haematuria is clot retention with urinary tract obstruction. Patients with significant bleeding may need a three-way catheter and continuous bladder irrigation. All patients should undergo renal tract imaging and cystoscopy to exclude malignancy or other serious causes. Avoid TXA as it can cause clot retention
📌 About
- Macroscopic haematuria: red urine visible to the naked eye. May be mimicked by haemoglobinuria, myoglobinuria, porphyrins, or bile pigments → confirm with microscopy.
- Microscopic haematuria: >3–5 RBCs per high-power field on urine microscopy.
- Heavy bleeding with clots can cause anaemia, hypotension, and bladder outlet obstruction.
- In patients >60 years, haematuria is a red flag for urinary tract cancer.
- Urology referral is mandatory in macroscopic haematuria and strongly advised in older patients with microscopic haematuria.
💡 Top Tips
- In a solitary kidney, adopt a lower threshold for inpatient investigation and urgent urology referral.
- Macroscopic haematuria with clots may mimic renal colic → take care not to miss obstruction.
- After pelvic trauma, blood at the meatus or perineal bruising suggests urethral injury. ➡️ Perform a retrograde urethrogram before attempting catheterisation. Early urology input essential.
🔎 Causes
- Malignancy: renal cell carcinoma, urothelial carcinoma (renal pelvis, ureter, bladder), prostate, urethra.
- Stones: renal or ureteric calculi.
- Infection: UTI, schistosomiasis.
- Trauma: blunt or penetrating.
- Benign prostatic hyperplasia (BPH).
- Exercise-induced haematuria (classically post-marathon; can be linked to IgA nephropathy).
- Haemorrhagic cystitis (e.g. cyclophosphamide), Endometriosis.
- Glomerular disease: IgA nephropathy, post-streptococcal GN, vasculitis.
- Post-urological procedures (e.g. TURP).
- Coagulopathy or over-anticoagulation.
- Vascular lesions (AV malformation, angiomyolipoma).
🎨 Other Causes of Red/Discoloured Urine
- Menstruation, Jaundice.
- Foods: beetroot, red cabbage.
- Dyes: paprika, artificial colourings.
- Drugs: rifampicin, metronidazole, nitrofurantoin, warfarin, phenytoin.
- Infections with indigo-positive bacteria (e.g. indoxyl sulphatase activity).
- Rhabdomyolysis (myoglobinuria).
- Metabolic: porphyria, alkaptonuria.
🧑⚕️ Clinical Assessment
- Ask: passage of clots, dysuria, frequency, urgency, incontinence.
- Systemic symptoms: fever (UTI), weight loss (malignancy), flank pain (stones).
- Occupational exposure (chemicals, dyes) & smoking history → ↑ risk of bladder TCC.
- Past medical history: bleeding disorders, anticoagulant use.
- Trauma history → avoid catheterisation until urethral injury excluded.
- Recent sore throat/URTI in young patients → think IgA nephropathy.
- Travel history → schistosomiasis → SCC bladder risk.
- Examination: palpable bladder (retention), abdominal mass, DRE, vaginal exam to localise bleeding.
- Note urine colour (rose, claret, “smoky” brown) and presence of clots → helps localisation (glomerular vs post-glomerular).
🧪 Investigations
- Bloods: FBC, U&E + eGFR, clotting screen, PSA (men), β-hCG (fertile females). Group & save if bleeding heavy.
- Urine: Dipstick, microscopy, MSSU.
- Imaging: – Ultrasound ± CT-KUB (stones, tumours). – Plain KUB X-ray (radio-opaque stones). – IVU now rarely used (contrast risk).
- Cystoscopy: gold standard for macroscopic haematuria.
📩 Nephrology Referral
- Proteinuria >2+ on dipstick.
- eGFR <60 mL/min/1.73m².
- Abnormal imaging consistent with intrinsic renal disease.
- Suspected primary renal pathology: IgA nephropathy, Alport’s, thin membrane disease, GN, ADPKD, vasculitis.
🩺 Three-Way Catheter
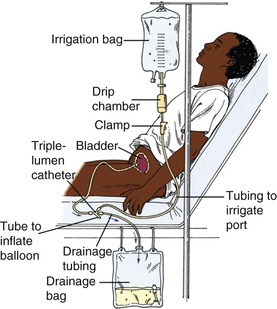
- Large bore (22–24 Fr) Foley.
- Ports: balloon inflation (20–30 ml water), urine drainage, irrigation fluid entry.
- Manual irrigation with 50 ml sterile water aliquots until clear, then set up continuous bladder irrigation.
⚡ Management
- Admit if: clot retention, haemodynamic instability, uncontrolled pain, sepsis, AKI, coagulopathy, heavy bleeding, severe comorbidity, or poor social support. Encourage high oral fluid intake if safe, to reduce clot formation. Avoid Tranexamic acid.
- Clot retention: insert 3-way catheter + continuous irrigation. If unavailable → large 2-way catheter (≥16 Ch) + manual irrigation, but definitive upgrade needed.
- Suprapubic catheter (SPC): irrigation possible if SPC already in place; avoid fresh insertion if bladder tumour suspected (risk of tumour seeding).
- Coagulopathy: correct anticoagulation as appropriate.
- If bleeding persists: urgent urology review ± surgical/endoscopic haemostasis.
- Blood transfusion if symptomatic anaemia.
- ⚠️ Avoid tranexamic acid → may worsen clot retention.
📚 References
📌 Revisions
- Streamlined with emphasis on red flags, three-way catheter technique, and referral thresholds.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery