Related Subjects:
|Cellulitis
|Pyoderma gangrenosum
|Pemphigus Vulgaris
|Toxic Epidermal Necrolysis
|Stevens-Johnson Syndrome
|Necrotising fasciitis
|Gas Gangrene (Clostridium perfringens)
|Purpura Fulminans
|Severe burns
|Anatomy of Skin
|Skin Pathology and Lesions
|Skin, Soft Tissue & Bone Infections
⚠️ Toxic Epidermal Necrolysis (TEN) is a rare, life-threatening dermatological emergency.
It lies at the most severe end of the SJS–TEN spectrum, caused by an immune-mediated reaction against keratinocyte adhesion molecules.
This leads to widespread skin necrosis, epidermal detachment, and mucosal involvement.
📌 About
- Part of the SJS–TEN spectrum (SJS: <10% BSA, TEN: >30% BSA, overlap: 10–30%).
- Marked by extensive epidermal sloughing, like a severe burn injury.
- High risk of sepsis, fluid loss, multi-organ failure, and death.
🧾 Aetiology
- 💊 Drug-induced (most common) – sulphonamides, cephalosporins, anticonvulsants (carbamazepine, phenytoin, lamotrigine).
- 🧬 Idiopathic cases → worse prognosis, esp. in haematological malignancy (e.g. leukaemia, lymphoma).
- 🦠 Higher risk in viral infections (notably HIV).
- 🧪 Genetic risk: slow acetylator phenotype predisposes.
💊 Common Culprit Drugs (≈50% cases)
- Allopurinol
- Carbamazepine / Lamotrigine
- Nevirapine
- Oxicam NSAIDs
- Phenobarbital
- Phenytoin
- Sulphonamides (e.g. sulfamethoxazole)
- Sulfasalazine
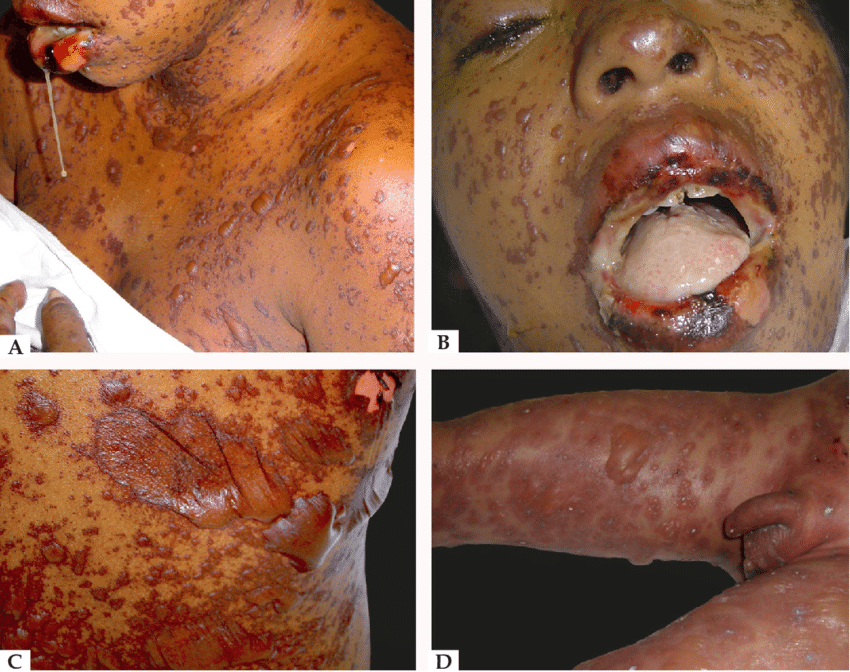
🤒 Clinical Features
- Prodrome: fever, malaise, myalgia (flu-like).
- Painful, rapidly spreading erythema → confluent blistering.
- Mucous membrane involvement: oral, ocular, genital.
- Widespread epidermal detachment → erosions, fluid loss, risk of infection.
- Sepsis & multi-organ failure are leading causes of death.
🔍 Differential Diagnosis
- Staphylococcal scalded skin syndrome (SSSS) – mucosa spared.
- Toxic shock syndrome.
- DRESS (Drug Reaction with Eosinophilia & Systemic Symptoms).
- Severe phototoxic reactions.
📊 SCORTEN Severity Score
- Age >40 years → +1
- HR >120 bpm → +1
- Underlying malignancy → +1
- BSA detachment >10% → +1
- Urea >10 mmol/L → +1
- HCO₃⁻ <20 mmol/L → +1
- Glucose >14 mmol/L → +1
💀 Mortality by SCORTEN
- 0–1 → ~3%
- 2 → ~12%
- 3 → ~35%
- 4 → ~58%
- ≥5 → ~90%
🧪 Investigations
- Bloods: FBC, U&E, LFTs, CRP, coagulation profile.
- Skin biopsy → differentiates TEN from SSSS.
- Blood & urine cultures; CXR if febrile.
🏥 Management
- 🔺 Admit ICU / burns unit if SCORTEN ≥2 or BSA >10% involved.
- ⚡ Supportive care: fluid/electrolyte balance, nutrition, thermoregulation.
- 🔥 Fire risk: paraffin-based emollients are flammable → CO₂ extinguisher + fire blanket at bedside.
- 🫁 Airway: anticipate obstruction if mucosa involved; use non-adhesive fixation.
- 💨 Breathing: monitor for ARDS; use lung-protective ventilation if intubated.
- 💉 Circulation: invasive access via unaffected skin; fluids, albumin, vasopressors as required.
- 🩸 Transfusion: maintain Hb >70 g/L (or >90 in CVD); monitor coagulopathy.
- 💊 Analgesia: opioids ± sedation for dressing changes; early pain team input.
- 🌡️ Exposure: prevent hypothermia (room 25–28°C; warmed IV fluids).
- 🥗 Nutrition: NG feeding early; consider parenteral if needed; beware refeeding syndrome.
- 🦠 Infection: barrier nursing; treat only proven infection (early Staph → later Gram-negatives like Pseudomonas).
- 👁️ Ophthalmology: daily review; lubricants ± topical antibiotics.
📚 References
🖼️ Images