
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Lungs
Related Subjects: |AP of the Lungs |AP of the Heart |Coronary AP |Cardiac Embryology |Gastrointestinal tract Physiology |Autonomic Nervous System
🫁 AP of the Lungs - In Depth (Makindo)
The lungs are paired, highly vascular, elastic organs primarily responsible for gas exchange, maintaining acid–base balance by eliminating CO2 (the major volatile acid), and contributing to metabolic functions (e.g., angiotensin conversion, arachidonic acid metabolism). They process ~8,000–10,000 L of air daily in adults at rest, achieving near-equilibrium oxygenation and CO2 removal. Optimal function depends on precise integration of ventilation (air movement), perfusion (blood flow), diffusion (gas transfer), and neural/chemical control mechanisms. Disruptions lead to common pathologies like COPD, ARDS, pneumonia, and pulmonary embolism.
🏗️ 1) Gross Anatomy and Organisation
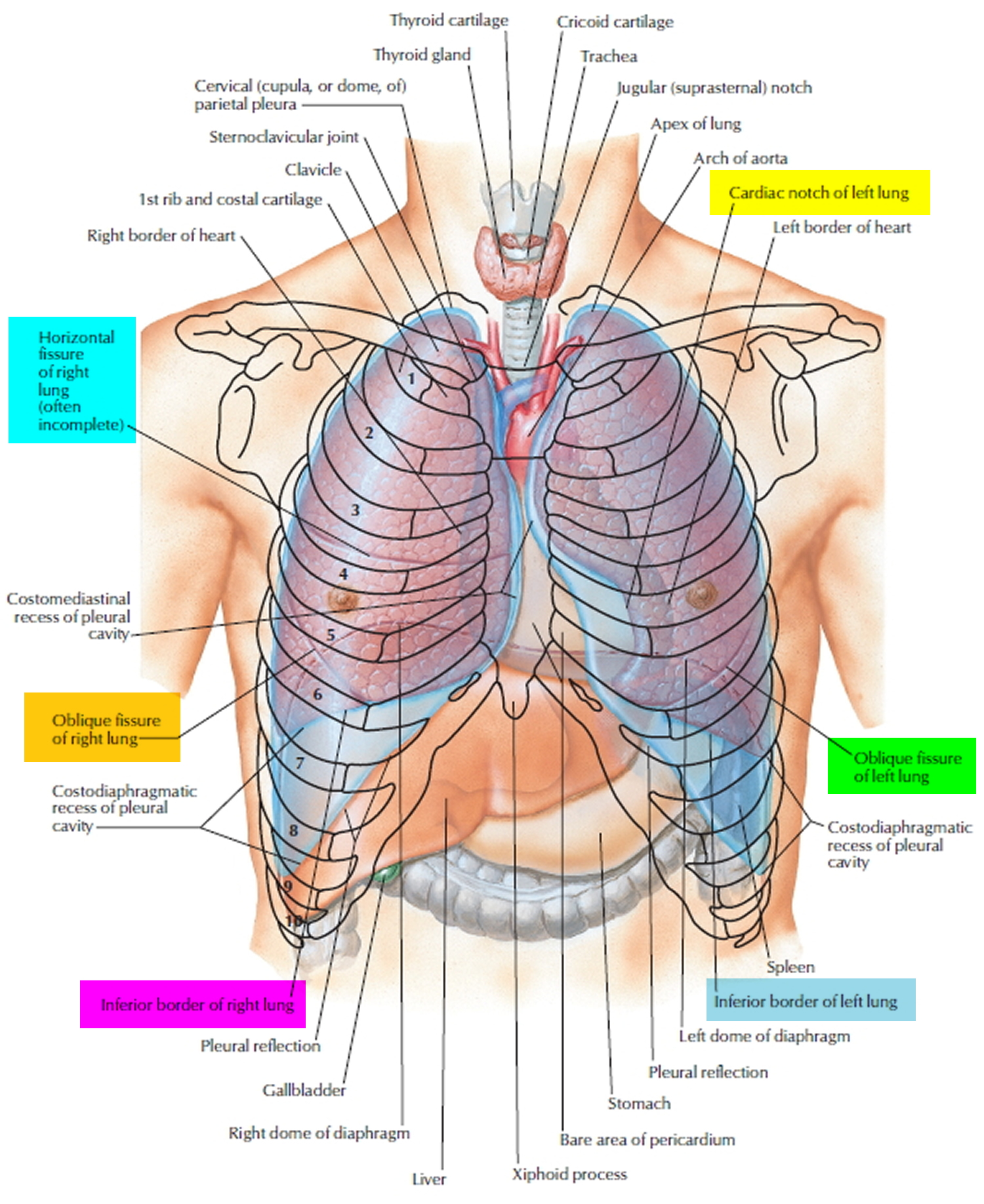
- Position and Shape: Lungs lie in pleural cavities flanking the mediastinum; cone-shaped with apex superior (extends 2–3 cm above 1st rib into supraclavicular fossa) and broad base resting on diaphragm. Right lung larger (~10% bigger) due to liver elevation; weighs ~625 g; left ~565 g. Cardiac notch on left anterior border accommodates heart.
- Surfaces: Costal (convex, rib impressions), mediastinal (concave with hilum impressions: heart, aorta, esophagus), diaphragmatic (concave, fits diaphragm dome), and sharp anterior/inferior borders.
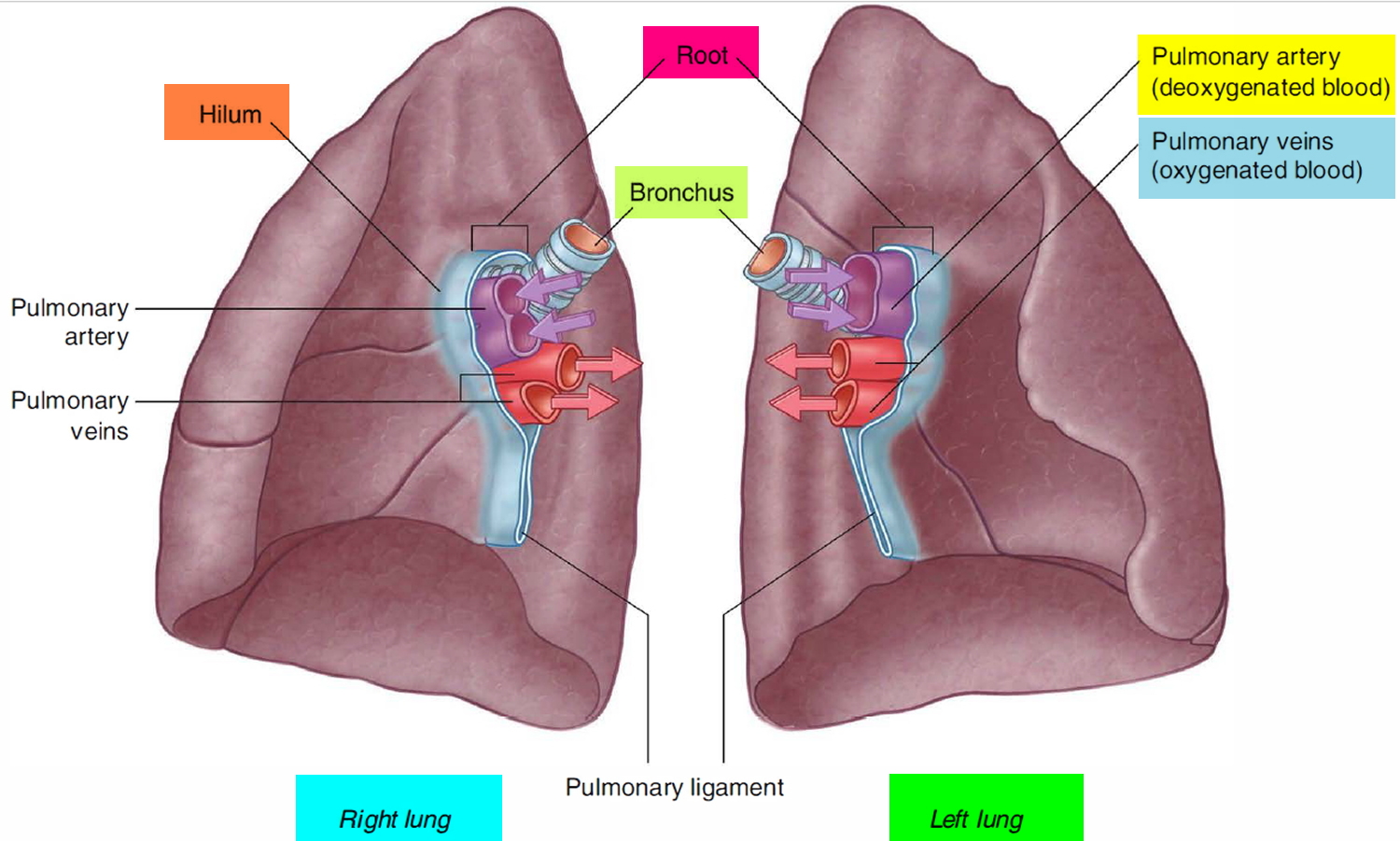
- Hilum (Root): Medial gateway; contains main bronchus (posterior), pulmonary artery (superior), two pulmonary veins (inferior), bronchial arteries/veins, lymph nodes/vessels, vagus/sympathetic nerves. Right hilum slightly higher.
- Blood Supply Overview: Dual: pulmonary (deoxygenated, low-pressure) and bronchial (oxygenated, systemic, high-pressure, ~1–2% cardiac output).
🧩 Lobes, Fissures, and Bronchopulmonary Segments
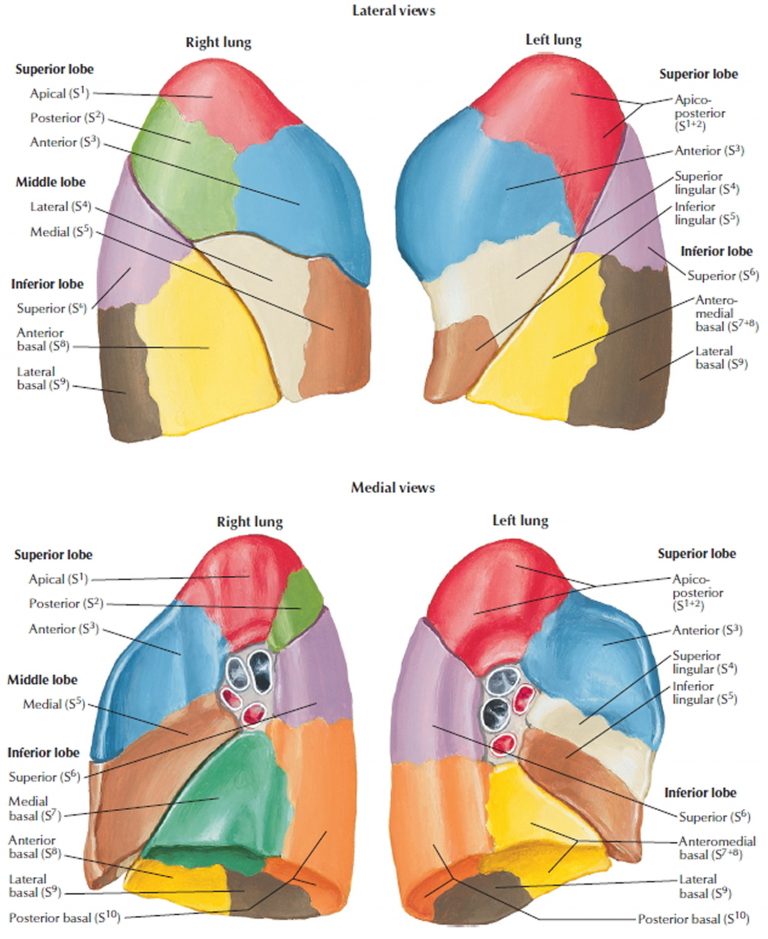
- Right lung: 3 lobes (superior, middle, inferior) separated by horizontal fissure (between superior/middle) and oblique fissure (between superior/middle and inferior). 10 bronchopulmonary segments: superior (apical, posterior, anterior), middle (lateral, medial), inferior (superior, medial basal, anterior basal, lateral basal, posterior basal).
- Left lung: 2 lobes (superior with lingula, inferior) separated by oblique fissure only. Lingula (tongue-like projection) analogous to right middle lobe. 8–10 segments (superior: apicoposterior, anterior, superior lingular, inferior lingular; inferior similar to right but fused basal segments).
- Bronchopulmonary Segments: Independent functional/surgical units; each with own segmental bronchus (from lobar), pulmonary artery branch, and segmental vein (drains to pulmonary veins). Separated by connective tissue planes with minimal collateral circulation.
📌 Clinical: Enables precise resections (segmentectomy for early lung cancer, bronchiectasis) while sparing healthy tissue. Segmental anatomy guides bronchoscopy and targeted therapies.
🫧 2) Pleura and Pleural Space
- Visceral Pleura: Thin serous layer tightly adherent to lung surface, fissures, interlobar surfaces; continuous with parietal at hilum; poor sensory innervation except near hilum (vagus/phrenic nerves).
- Parietal Pleura: Lines thoracic cavity: costal (ribs/intercostals), diaphragmatic (diaphragm), mediastinal (mediastinum/pericardium), cervical (neck). Rich sensory supply (phrenic for diaphragmatic/mediastinal → referred shoulder pain; intercostal for costal).
- Pleural Space: Potential space (~10–20 mL fluid total); negative pressure maintained by lymphatic drainage and Starling forces; fluid turnover ~0.5 mL/h.
- Intrapleural Pressure Dynamics: Resting -5 cmH₂O; inspiration -8 to -10 cmH₂O (diaphragm descent); forced expiration positive. Couples lung to chest wall expansion.
📌 Clinical: Pneumothorax → atmospheric pressure equilibration → lung collapse (atelectasis). Tension pneumothorax → progressive pressure rise → mediastinal shift, vena cava compression, hypotension/shock. Pleural effusion (>300 mL) → restrictive defect, reduced FRC, dyspnea.
🌳 3) The Airway Tree - Conducting vs Respiratory Zones
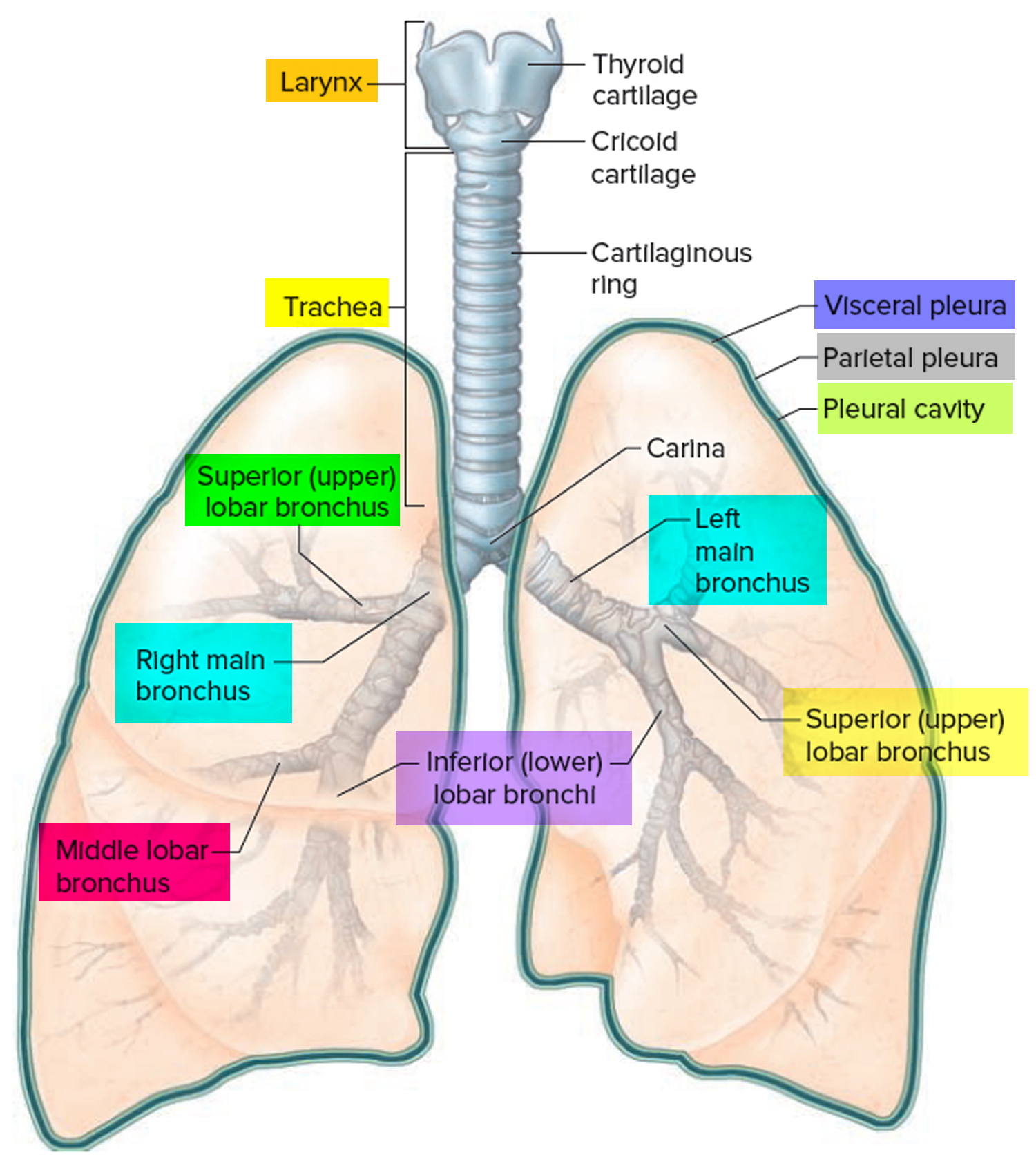
- Conducting Zone (0–16 generations): Trachea → main bronchi → lobar → segmental → bronchioles → terminal bronchioles. No gas exchange; warms/humidifies/filters air; anatomical dead space ~150 mL (2 mL/kg). Cartilage in larger airways prevents collapse; smooth muscle increases distally.
- Respiratory Zone (17–23 generations): Respiratory bronchioles (first alveoli) → alveolar ducts → alveolar sacs → alveoli. ~300–480 million alveoli; surface area 50–100 m²; primary gas exchange site.
🔎 Trachea and Main Bronchi
- Trachea: 10–12 cm long, 2–2.5 cm diameter; 16–20 C-shaped hyaline cartilage rings (open posteriorly); trachealis muscle (smooth) allows esophageal expansion; bifurcates at carina (T4/T5 vertebral level, descends ~2 cm on deep inspiration).
- Right Main Bronchus: Shorter (~2.5 cm), wider, steeper angle (~25° from vertical) → higher aspiration risk (foreign bodies, aspiration pneumonia often right-sided).
- Left Main Bronchus: Longer (~5 cm), narrower, more horizontal (~45° angle); crosses under aortic arch.
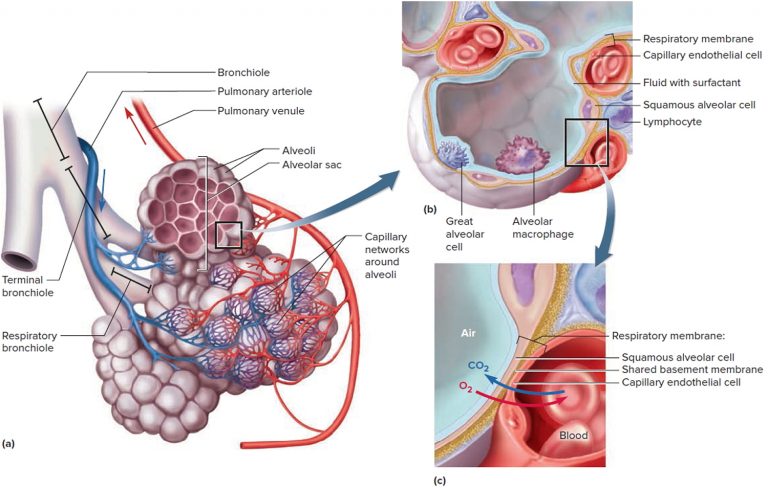
🧬 4) Microanatomy of the Alveoli
- Alveoli: Thin-walled polyhedral sacs (~250–300 μm diameter); ~300–480 million; total surface ~70–100 m² in adults; walls contain elastic fibers for recoil.
- Type I Pneumocytes: Flat squamous cells (cover ~95% surface area); thin cytoplasm (0.1–0.2 μm) for minimal diffusion barrier; tight junctions prevent fluid leak.
- Type II Pneumocytes: Cuboidal; ~5% surface; synthesize/store surfactant in lamellar bodies; can proliferate to repair type I damage (stem-like function); express aquaporins for fluid balance.
- Alveolar Macrophages: Mobile phagocytes derived from monocytes; clear debris, pathogens, surfactant; iron-laden in smokers ("smoker's macrophages").
- Alveolar–Capillary Membrane: ~0.2–0.5 μm thick (type I + basement membrane + endothelium); pores of Kohn allow collateral air flow; tight junctions limit protein leak.
🫧 Surfactant (Critical Stabilizer)
Surfactant (~90% phospholipids like dipalmitoylphosphatidylcholine, 10% proteins A–D) lowers surface tension dynamically (more in smaller alveoli per Laplace’s law: P = 2T/r), preventing atelectasis, reducing work of breathing by ~50–70%, and stabilizing alveoli during expiration. Type II cells produce ~10–20 mg/kg/day. Deficiency → neonatal RDS (prematurity), ARDS (inactivation by inflammation/protein leak) → stiff lungs, high ventilator pressures, barotrauma risk.
🩸 5) Pulmonary and Bronchial Circulations
- Pulmonary Circulation: Low-resistance, high-capacitance (~500–1000 mL blood volume); right ventricle → pulmonary trunk → arteries → alveolar capillary network (sheet flow) → veins → left atrium. Mean pressure ~15 mmHg; accommodates full cardiac output with minimal pressure rise.
- Bronchial Circulation: Systemic (aortic branches); supplies airways to terminal bronchioles, supporting structures, visceral pleura (~1–2% cardiac output); venous drainage mixes with pulmonary veins (physiological shunt ~1–2%).
- Hypoxic Pulmonary Vasoconstriction (HPV): Local response to low alveolar PO₂ (<70 mmHg) → vasoconstriction diverts blood to better-ventilated areas; optimizes V/Q; inhibited by volatiles, alkalosis.
📌 Clinical: Pulmonary embolism → acute dead space increase, hypoxemia, right heart strain. Chronic hypoxia → persistent HPV → pulmonary hypertension → cor pulmonale.
⚙️ 6) Mechanics of Breathing
- Inspiration: Active; diaphragm (primary, 75% tidal volume), external intercostals, scalenes/accessories → thoracic volume ↑ → intrapleural pressure ↓ → alveolar pressure negative → airflow in.
- Expiration: Passive (elastic recoil dominant at rest); active in forced breathing (internal intercostals, abdominals).
- Elastic Recoil: Lung inward (elastin + surface tension ~2/3); chest wall outward; balanced at FRC.
- Airway Resistance: ~80% in medium/large airways; Poiseuille’s law (R ∝ 1/r⁴) explains dramatic rise in asthma/COPD.
🧮 Lung Compliance - Detailed Physiology
Lung compliance quantifies distensibility: ability to expand with pressure change. C = ΔV / ΔP (mL/cmH₂O). Normal static lung compliance ~200 mL/cmH₂O; total respiratory system ~70–100 mL/cmH₂O.
- Types: Static (no flow, elastic only); Dynamic (includes resistance); Specific (per unit volume).
- Factors: Surfactant (major ↑); elastin/collagen; chest wall; volume (sigmoid P-V curve, peak mid-range); age (↓); posture (supine ↓ FRC/compliance).
- Clinical: ↑ in emphysema (loss recoil → hyperinflation); ↓ in fibrosis/ARDS/pneumonia (stiff → ↑ work, high pressures).
- Measurement: Ventilator: C_stat = TV / (P_plateau - PEEP); C_dyn = TV / (P_peak - PEEP). P-V loops show hysteresis (surfactant).
📦 7) Lung Volumes, Capacities, and Dead Space
- Tidal Volume (TV): 500 mL (~7 mL/kg).
- Inspiratory/Expiratory Reserve Volumes (IRV/ERV): ~3 L / ~1.2 L.
- Residual Volume (RV): ~1.2 L (prevents collapse).
- Vital Capacity (VC): ~4.8 L; Total Lung Capacity (TLC): ~6 L.
- Functional Residual Capacity (FRC): ~2.4 L (ERV + RV); buffer zone; ↓ in obesity/anesthesia → atelectasis.
- Dead Space: Anatomical ~150 mL; physiological (includes alveolar) ~30% TV normally; ↑ in PE, low cardiac output.
📌 Clinical: Obstructive disease ↑ RV/TLC ratio; restrictive ↓ VC/TLC. PEEP recruits alveoli, ↑ FRC, improves oxygenation.
🌬️ 8) Gas Exchange and V/Q Matching
- Diffusion: Fick’s law; O₂ limited by perfusion normally; CO₂ ~20× more soluble.
- V/Q Ratio: Ideal ~0.8; gravity creates apex high V/Q (~3), base low (~0.6).
- Zones (West): Zone 1 (dead space-like, rare); Zone 2 (intermittent flow); Zone 3 (continuous, base).
Shunt (V/Q=0): atelectasis/pneumonia → refractory hypoxemia. Dead space (V/Q=∞): PE → hyperventilation, normal/high PaO₂ but ↑ A-a gradient.
🩸 9) Oxygen and CO₂ Transport
🟦 Oxygen Transport
- ~97% Hb-bound (1.34 mL O₂/g Hb); 3% dissolved.
- Sigmoid curve (cooperative binding); P50 ~27 mmHg.
- Bohr effect: right shift (acidosis, hypercapnia, fever, 2,3-DPG) → tissue unloading.
🟩 Carbon Dioxide Transport
- ~70% bicarbonate (carbonic anhydrase in RBCs); 23% carbamino-Hb; 7% dissolved.
- Haldane effect: deoxy-Hb carries more CO₂.
🧠 10) Control of Ventilation
- Rhythm Generators: Pre-Bötzinger complex (medulla).
- Chemoreceptors: Central (CO₂/pH via CSF, 70–80% drive); Peripheral (carotid/aortic, hypoxic when PaO₂ <60 mmHg).
- Other: Stretch (Hering-Breuer), irritant, J-receptors, cortical/voluntary.
In chronic hypercapnia (COPD), hypoxic drive predominates - supplemental O₂ risks CO₂ retention via V/Q worsening + minor drive loss.
🛡️ 11) Lung Defence Mechanisms
- Mucociliary clearance (5–20 mm/min); cough; alveolar macrophages; IgA, defensins, collectins.
Impaired in smoking (cilia paralysis), CF (thick mucus), immunosuppression → infection risk.
🩺 12) Clinical Correlations (Physiology to Bedside)
- Asthma: ↑ resistance, reversible.
- COPD: Emphysema (↓ recoil, ↑ compliance); chronic bronchitis (mucus).
- Fibrosis/ARDS: ↓ compliance, diffusion barrier.
- PE: Dead space, V/Q mismatch.
- Pneumonia: Shunt.
📊 Summary (High-Yield Integration)
Lungs excel through matched ventilation-perfusion-diffusion, governed by mechanics (compliance/recoil/resistance) and precise control. Failures stem from disrupted components: obstruction (airflow), alveolar filling/collapse (diffusion/shunt), vascular occlusion (dead space), or control issues. Master V/Q as the unifying principle.
💡 Teaching Tip: Lungs = “pump (mechanics) + filter (alveoli/capillaries) + controller (chemoreflexes)”. Pathology = which breaks and how it skews V/Q/gas exchange.