
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Ankylosing spondylitis
Related Subjects: |Monoarticular arthritis |Polyarticular arthritis |Seronegative Spondyloarthropathies |Ankylosing spondylitis |Enteropathic Spondyloarthritis |Reactive Arthritis |Psoriatic Arthritis |Adult Onset Still's Disease |Alkaptonuria
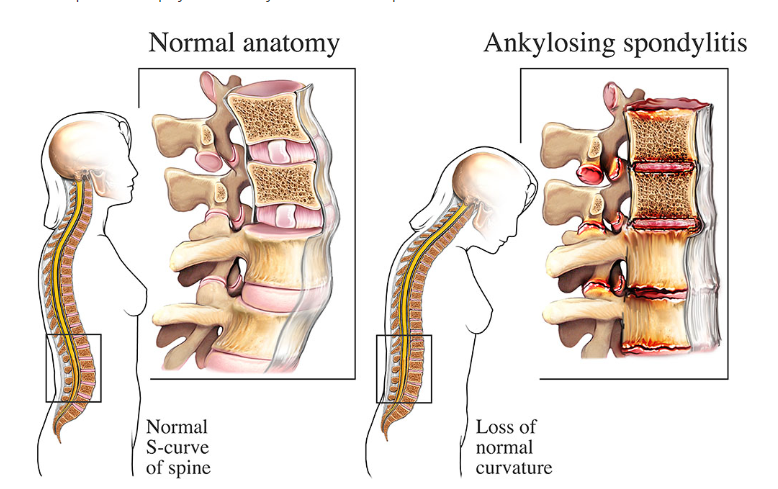
🦴 Ankylosing Spondylitis (AS) is a chronic, progressive inflammatory disease of the axial skeleton. It causes loss of lumbar lordosis, ↑ thoracic kyphosis, and sacroiliitis, with systemic extra-articular features. 💡 Classic: young man with back pain + morning stiffness that improves with exercise but not rest! 🏃♂️
ℹ️ About
- Part of the seronegative spondyloarthritides (RF negative, HLA-B27 linked).
- Onset: age 15–40, male:female ≈ 4:1.
- Inflammatory back pain starts in sacroiliac joints → ascends spine.
- Associated with enthesitis, peripheral arthritis, and systemic features.
⚙️ Pathology
- Chronic enthesitis (inflammation where ligaments/tendons attach to bone).
- New bone formation → syndesmophytes → gradual spinal fusion (bamboo spine on X-ray).
- Loss of lumbar lordosis, ↑ thoracic kyphosis, fixed flexion deformity.
- Costovertebral joint involvement → ↓ chest expansion.
🧬 Aetiology
- Strong genetic link: HLA-B27 present in >90% of patients.
- Environmental/infective triggers suggested (e.g. Klebsiella pneumoniae molecular mimicry).
📊 HLA-B27 Association
- Caucasian general population: ~8% carry HLA-B27.
- Ankylosing spondylitis: 90%.
- Reactive arthritis (Reiter’s): 70%.
- Enteropathic arthritis: 50%.
- Psoriatic arthritis: 20%.
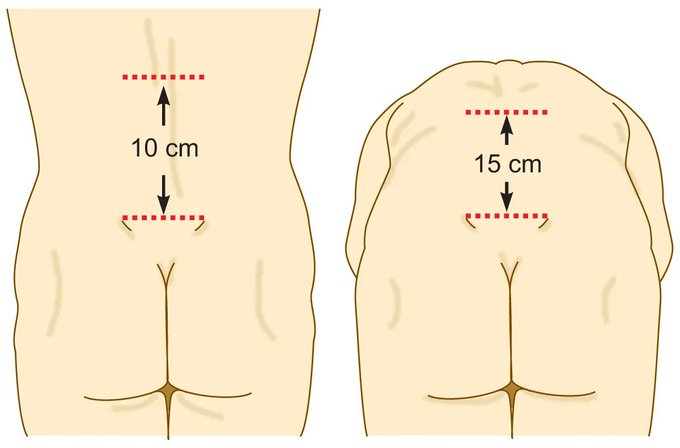
Modified Schober Test
👨⚕️ Clinical – Spinal
- Young male, insidious onset chronic low back pain + morning stiffness >1h.
- Symptoms improve with exercise, not with rest.
- Loss of lumbar lordosis, ↑ thoracic kyphosis → “question-mark posture ❓”.
- Alternating buttock pain (sacroiliitis).
- Spinal rigidity → risk of fractures, cauda equina, cord compression.
🌍 Clinical – Extra-articular
- 👁️ Acute anterior uveitis (red, painful eye, photophobia, blurred vision).
- ❤️ Aortic regurgitation, aortitis, AV block.
- 🫁 Apical pulmonary fibrosis → restrictive lung disease.
- 🦵 Peripheral arthritis (hips, shoulders); enthesitis (Achilles, plantar fascia).
- 🧪 Rare: secondary AA amyloidosis.
📝 Aide-Mémoire – “9 A’s”
- Ankylosis (spinal fusion)
- Anterior uveitis
- Amyloidosis
- Aortic regurgitation / Aortitis
- AV block
- Apical pulmonary fibrosis
- Achilles tendonitis
- Anderson lesion (spinal fracture)
- Anti-TNF therapy (treatment)
📏 Clinical Tests of Spinal Mobility
- Modified Schober Test: lumbar flexion ↑ >3 cm normally.
- Lateral flexion: fingertip–floor distance ↓ >10 cm.
- Chest expansion: normally >3 cm at 4th intercostal space.
- Occiput–wall distance: normally 0 cm.
- Chin–sternum distance: should touch sternum.
- Cervical rotation: >50° normally.
- Intermalleolar distance: reduced if hip involvement.
🔎 Investigations
- Inflammatory markers: ESR, CRP often ↑.
- HLA-B27: supportive but not diagnostic.
- X-ray pelvis: bilateral sacroiliitis, squaring of vertebrae, syndesmophytes → “bamboo spine”.
- MRI sacroiliac joints: detects early inflammation before X-ray changes.
💊 Management
- 🏃 Physiotherapy + exercise: cornerstone of management.
- 💊 NSAIDs (naproxen, indomethacin) first-line for pain/stiffness.
- 🧴 Biologics: anti-TNF (etanercept, adalimumab) or IL-17 inhibitor (secukinumab) if refractory.
- 💊 DMARDs (e.g. sulfasalazine, methotrexate): helpful for peripheral arthritis, not axial disease.
- 🦴 Bisphosphonates if osteoporosis risk.
- 👁️ Treat uveitis promptly with steroids (ophthalmology input).
- 💉 Surgery: joint replacement if severe hip involvement.
📚 Teaching Pearls
💡 Key exam clue = young man + inflammatory back pain that improves with activity. 🔍 Always check for extra-articular features (esp. uveitis, cardiac). ⚠️ Complication to remember = spinal fractures + cauda equina. 🏥 Long-term monitoring: bone density, echo (aortic regurg), chest imaging, ophthalmology.
Cases - Ankylosing Spondylitis (AS)
- Case 1 - Classic young man with back pain 🧍♂️: A 24-year-old man presents with 1 year of progressive low back pain and stiffness, worse in the mornings and improving with activity. Exam: reduced lumbar flexion (positive Schober’s test) and tenderness over sacroiliac joints. X-ray: sacroiliitis. HLA-B27 positive. Diagnosis: ankylosing spondylitis. Managed with exercise and NSAIDs.
- Case 2 - Extra-articular features 👁️: A 32-year-old man with known AS develops acute painful red eye with photophobia. Exam: reduced vision and ciliary injection → acute anterior uveitis. Treated urgently with topical steroids and ophthalmology referral. His AS is escalated to biologic therapy (anti-TNF).
- Case 3 - Advanced disease 🦴: A 45-year-old man presents with progressive spinal stiffness and limited chest expansion. Lateral spine X-ray shows “bamboo spine” from syndesmophyte formation. He also has restrictive lung defect on spirometry. Managed with physiotherapy, biologics, and respiratory support as needed.
Teaching Point 🩺: Ankylosing spondylitis is a seronegative spondyloarthropathy (HLA-B27 associated) with hallmark inflammatory back pain, sacroiliitis, and extra-articular features (uveitis, aortitis, restrictive lung disease). Early physiotherapy and biologics are key to improving outcomes.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery