
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Benign Paroxysmal Positional Vertigo (BPPV)
Related Subjects: |Assessing Hearing Loss |Benign Paroxysmal Positional Vertigo (BPPV) |Cholesteatoma |Epistaxis (Nosebleeds) |Acute Mastoiditis |Nasal polyps |Acute Sinusitis |Sudden Sensorineural Hearing loss (SNHL) |Causes of Vertigo
💡 BPPV is the most common cause of vertigo. It is due to displaced otoconia (calcium carbonate crystals) within semicircular canals. Symptoms are brief but disabling, and correct diagnosis plus repositioning maneuvers (Epley) are highly effective.
📖 About
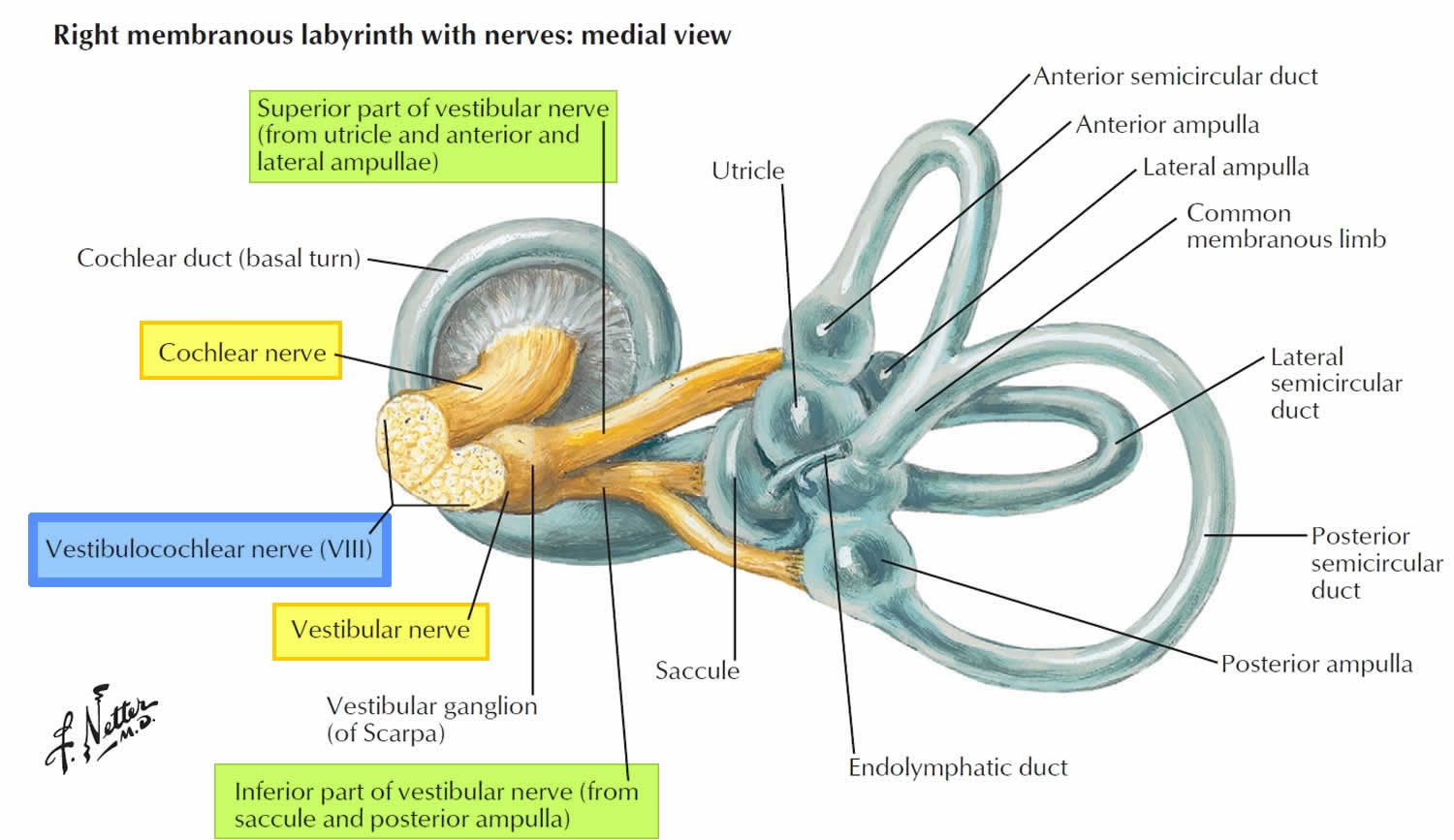
- Canalithiasis = free-floating calcium carbonate crystals from the utricle enter the semicircular canals.
- They disturb normal endolymph flow → inappropriate stimulation of hair cells → vertigo & nystagmus.
- Most common in adults aged 50–70 but can occur at any age.
🧬 Aetiology
- ~80% involve the posterior semicircular canal.
- 5–10% involve the horizontal canal (usually more intense vertigo).
- Can follow head trauma, viral infections, or occur idiopathically.
📊 Types of BPPV
- Posterior Canal BPPV (most common).
- Horizontal Canal BPPV.
- Anterior Canal BPPV (rare).
🩺 Clinical Features
- Acute vertigo triggered by head movement (e.g. turning over in bed).
- Attacks last < 1 minute.
- Often recurrent, may follow minor trauma or vestibular insult.
- No hearing loss or tinnitus (distinguishes from Ménière’s).
🔎 Diagnosis
- Diagnosis is clinical based on history + positional testing.
- Dix–Hallpike Test: induces vertigo + nystagmus if posterior canal BPPV. Watch demonstration.
- CT/MRI if atypical features or suspicion of brainstem/cerebellar lesion or acoustic neuroma.
⚖️ Differentials
- BPPV: Recurrent, brief, position-triggered vertigo, +ve Dix–Hallpike.
- Labyrinthitis: Severe acute vertigo, post-viral, often with hearing loss.
- Ménière’s disease: Vertigo + tinnitus + fluctuating hearing loss.
- Vestibular neuronitis: Prolonged vertigo days, no hearing loss.
- Acoustic neuroma: Progressive vertigo + unilateral hearing loss/tinnitus.
- Stroke / MS: Persistent vertigo + neurological signs.
- Vestibular migraine: Vertigo with headache/aura, spontaneous remission.
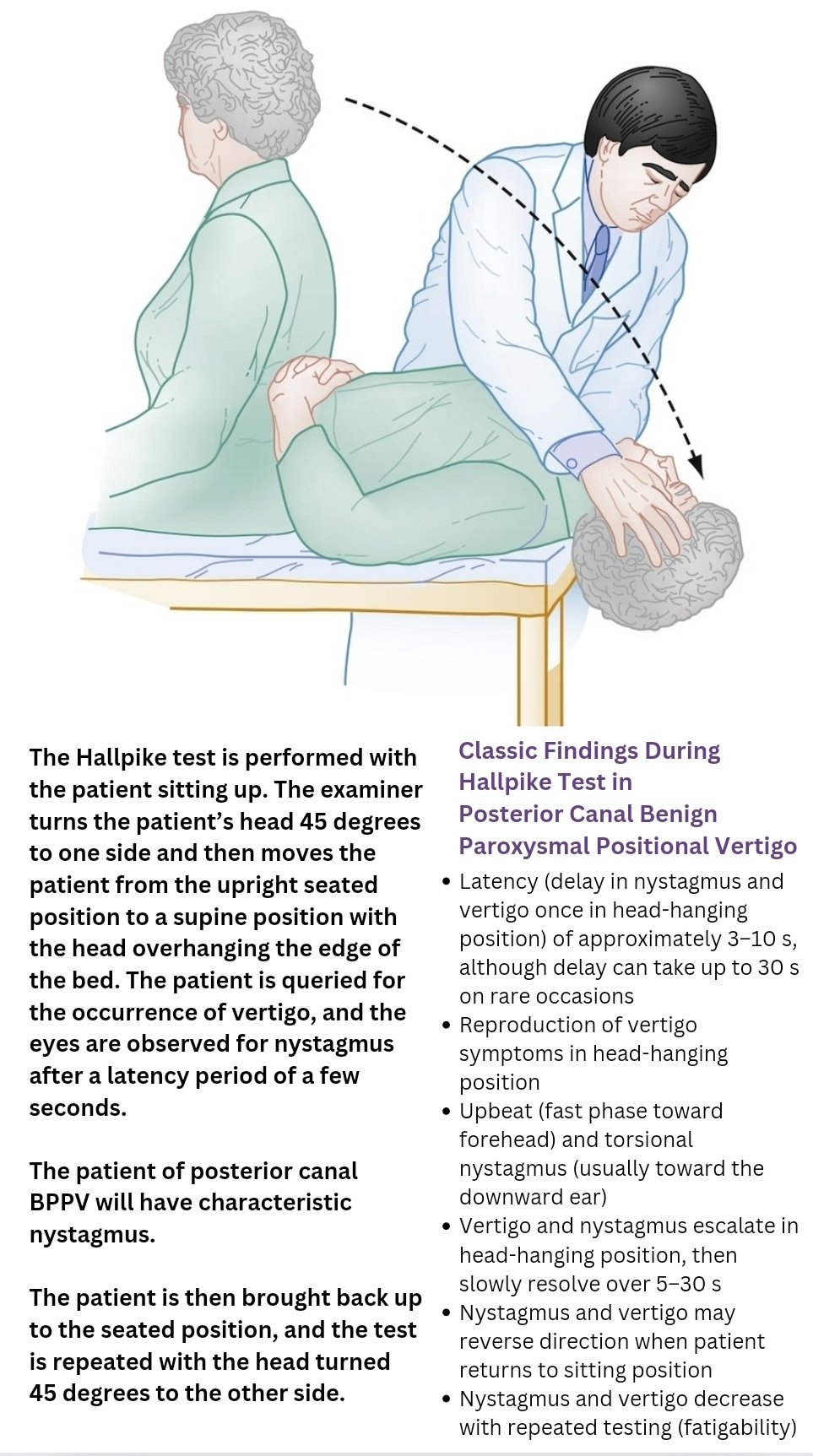
🧪 Dix–Hallpike Test
- Warn patient test may provoke vertigo.
- Patient sits upright, head turned 45° to one side.
- Lie patient back quickly with neck extended ~30° below horizontal.
- Look for vertigo + torsional nystagmus (latency 5–10 sec, fatigable, transient).
- Repeat on opposite side if negative.
💊 Management
- Definitive: Epley maneuver (posterior canal) – canalith repositioning back into utricle.
- Symptomatic relief: Short-term vestibular suppressants (cinnarizine, betahistine, hyoscine) if vertigo severe.
- Education: Reassure recurrence is common but benign; driving may be unsafe until controlled.
- Referral: ENT/vestibular physiotherapy if persistent or diagnosis uncertain.
🧑⚕️ Case Example
👩🦳 A 62-year-old woman presents with sudden episodes of spinning dizziness lasting < 1 minute, especially when rolling over in bed or looking up to a high shelf. She feels nauseated but has no hearing loss or tinnitus. On examination, the Dix–Hallpike test reproduces her vertigo and reveals a torsional nystagmus. 👉 Diagnosis: Posterior canal BPPV. ✅ Managed effectively with an Epley maneuver, and she is reassured about the benign but recurrent nature of the condition.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery