
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Intussusception in Adults
Related Subjects: |Rectal Prolapse |Anal Cancer |Anal Fissure |Intussusception in Adults |Pilonidal Abscess (sinus) |Haemorrhoids (Piles) |Angiodysplasia |Hartmann's procedure
Adult intussusception is a rare but important cause of bowel obstruction. Unlike in children-where most cases are idiopathic-adults nearly always have an underlying pathology such as a tumour, polyp, or adhesion acting as a “lead point.” Prompt recognition is vital because delays can lead to ischaemia, necrosis, and perforation.
ℹ️ About
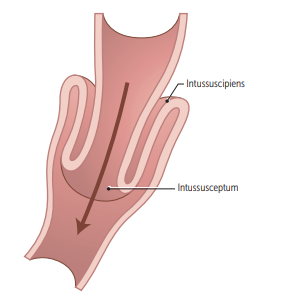
- Definition: Invagination of a proximal bowel segment into a distal segment, leading to obstruction and vascular compromise.
- Terminology: From Latin intus (“within”) and suscipere (“to receive”).
- Mechanism: A mass or irritant alters peristalsis, causing telescoping and progressive compromise of blood supply.
Epidemiology
- Rare: ~5% of all intussusceptions.
- Accounts for ~1% of adult bowel obstructions.
- Peak incidence: middle-aged to older adults.
🧬 Aetiology
- Tumours: Adenocarcinoma, lymphoma, metastases, gastrointestinal stromal tumour (GIST).
- Benign lesions: Polyps, lipomas, Meckel’s diverticulum.
- Postsurgical changes: Adhesions, bariatric (gastric bypass) or bowel surgery.
- Inflammatory conditions: Crohn’s disease or infection causing mucosal thickening.
Sites of Involvement
- Small bowel (52%):
- Enteroenteric – 39%
- Ileocolic – 13%
- Large bowel (38%):
- Ileocecal – 17%
- Colocolic – 17%
- Appendiceal – 4%
🩺 Clinical Features
- Often subacute or chronic – symptoms may last weeks to months before diagnosis.
- Colicky abdominal pain ± palpable mass.
- Obstructive features: Nausea, vomiting, constipation, distension.
- Red flag signs: Melaena, weight loss, systemic symptoms (may indicate malignancy).
- Some present acutely with peritonitis if perforation occurs.
🔎 Investigations
- Blood tests: FBC (↑WCC), U&Es (dehydration, electrolyte imbalance).
- X-ray: Dilated loops, air-fluid levels – non-specific.
- Ultrasound: “Target” or “doughnut” sign.
- CT scan (gold standard): Sausage-shaped or target mass, identifies lead point.
- Colonoscopy: May detect intraluminal masses but not first-line in acute obstruction.
💊 Management
- Stabilisation: IV fluids, NG tube, analgesia, antibiotics if sepsis suspected.
- Definitive treatment:
- Surgical resection (preferred) – avoids reducing a malignant lesion and missing pathology.
- Exploratory laparotomy or laparoscopy to inspect the entire bowel (from ligament of Treitz to terminal ileum).
- Endoscopic reduction considered in select benign cases, but uncommon in adults.
Prognosis
Outcome depends on the underlying cause. Benign lesions carry an excellent prognosis post-resection. Malignant causes account for the majority of large-bowel intussusceptions in adults, and prognosis depends on stage of disease at resection. Early recognition prevents catastrophic complications such as infarction and perforation.
References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery