
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Multiple Sclerosis (MS) ✅
Related Subjects: |Anatomy and Physiology of the Brain |Clinically Isolated Syndrome (CIS) |Focal Cortical Dysplasia (FCD) |Infantile Spasms (West Syndrome) |Neurological History taking |Motor Neuron Disease (MND-ALS) |Miller-Fisher syndrome |Guillain Barre Syndrome |Multifocal Motor Neuropathy with Conduction block |Multiple Sclerosis (MS) Demyelination |Transverse myelitis |Acute Disseminated Encephalomyelitis |Progressive Multifocal Leukoencephalopathy (PML) |Inclusion Body Myositis |Cervical spondylosis |Anterior Spinal Cord syndrome |Central Spinal Cord syndrome |Brown-Sequard Spinal Cord syndrome |Spinal Cord Compression |Spinal Cord Haematoma |Spinal Cord Infarction
🧠 Multiple sclerosis (MS) is a chronic, immune-mediated disease of the central nervous system causing inflammatory demyelination, axonal injury and progressive neurological disability. 📌 Modern diagnosis is based on a typical clinical syndrome plus supportive MRI/CSF evidence, while carefully excluding mimics such as NMOSD, MOGAD, infection, B12 deficiency, sarcoidosis, vasculitis and syphilis.
📊 Epidemiology
- 👥 Common cause of neurological disability in young and middle-aged adults.
- 🚶♀️ One of the commonest causes of serious physical disability in working-age adults.
- ⚖️ More common in women than men.
- ☀️ More common at higher latitudes, with vitamin D, EBV, smoking and genetic susceptibility implicated.
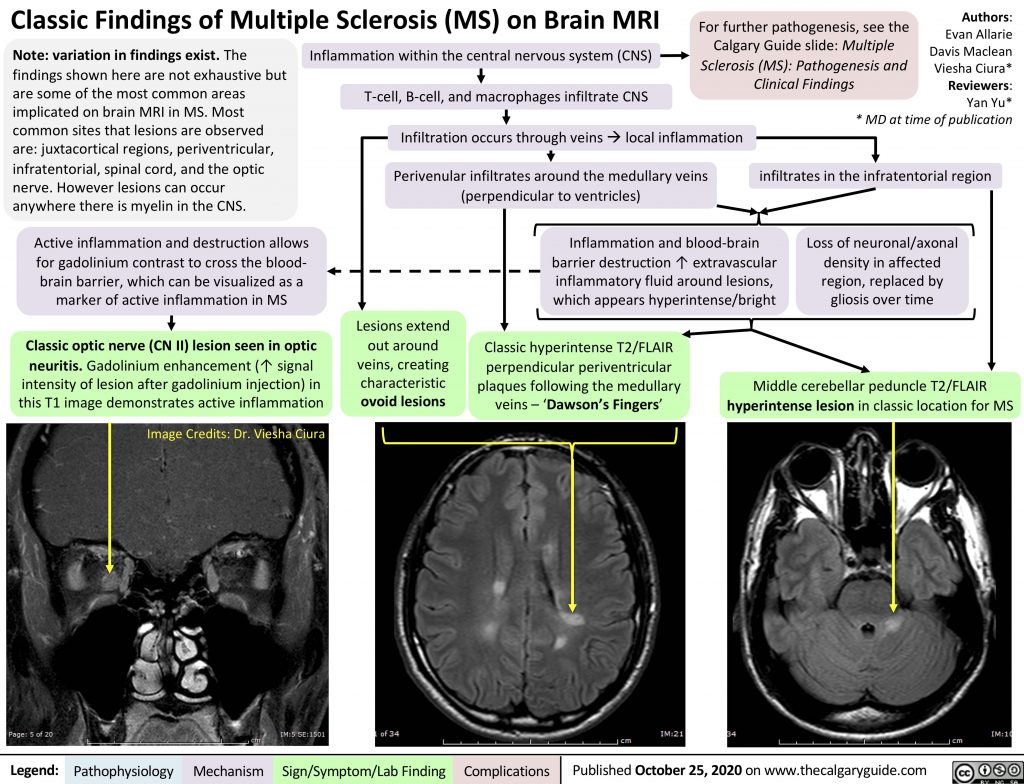
🔬 Pathology
- MS causes focal inflammatory demyelinating plaques in the CNS.
- Inflammation involves T cells, B cells, plasma cells, macrophages/microglia and complement.
- Myelin loss impairs saltatory conduction, causing conduction block and neurological symptoms.
- Axons may be relatively preserved early, but axonal injury contributes to permanent disability.
- Common plaque locations include:
- 🧠 Periventricular white matter
- 🧠 Juxtacortical / cortical regions
- 🎯 Infratentorial regions — brainstem and cerebellum
- 🧵 Spinal cord, especially cervical cord
- 👁️ Optic nerve — now recognised as an important demyelinating location in updated diagnostic criteria
🩺 Clinical Presentation
- Symptoms are usually CNS-localising, often subacute, evolving over hours to days and lasting more than 24 hours.
- Relapses may affect vision, sensation, motor function, coordination, brainstem function, bladder function or cognition.
- Symptoms may improve partially or completely, especially early in the disease.
- Progressive MS may present with gradual worsening gait, spastic paraparesis, imbalance or bladder dysfunction over months to years.
🧩 Typical Clinical Features
| Site / syndrome | Features |
|---|---|
| 👁️ Optic neuritis |
|
| 🧵 Myelitis |
|
| 🎯 Brainstem |
|
| 🌀 Cerebellar |
|
| ⚡ Sensory |
|
| 💤 Fatigue / cognition |
|
| 🔥 Uhthoff’s phenomenon |
|
🌀 Clinical Course / Forms of MS
- Relapsing-remitting MS: relapses with partial or complete recovery between attacks.
- Secondary progressive MS: gradual disability progression after an earlier relapsing-remitting phase.
- Primary progressive MS: progressive disability from onset, usually over at least 12 months.
- Fulminant / aggressive MS: rapid accumulation of disability; requires urgent specialist management.
📏 Diagnosis — Updated McDonald Criteria Concepts
🧠 2024 McDonald criteria update: diagnosis is moving away from a rigid “CIS/RIS first” framework. MS can be diagnosed earlier when the clinical picture is typical and there is supportive MRI or CSF evidence. Dissemination in time is no longer always essential if other highly supportive features are present.
| Concept | Explanation |
|---|---|
| Dissemination in space |
Lesions occur in typical CNS regions. Updated anatomical locations include:
|
| Dissemination in time | Historically required clinical attacks or MRI lesions at different times. In updated criteria, DIT is not always mandatory where other supportive biomarkers strongly support MS. |
| CSF oligoclonal bands | CSF-restricted oligoclonal IgG bands support chronic CNS inflammation and may substitute for DIT in appropriate clinical settings. |
| Kappa free light chain index | An emerging quantitative CSF marker of intrathecal immunoglobulin synthesis; included in the updated diagnostic framework as an alternative supportive CSF biomarker. |
| Central vein sign | MRI feature where a small vein is seen centrally within a white-matter lesion. It supports MS because MS lesions are characteristically perivenular. |
| Paramagnetic rim lesion | MRI feature suggesting chronic active inflammation at the edge of a lesion. It has high specificity for MS when present, but requires appropriate susceptibility-sensitive MRI sequences. |
🧪 Investigations
- MRI brain and spinal cord with contrast is the key investigation.
- MRI looks for demyelinating lesions in typical locations: periventricular, juxtacortical/cortical, infratentorial, spinal cord and optic nerve.
- Gadolinium enhancement suggests active inflammation.
- T1 black holes suggest more severe tissue injury / axonal loss.
- Central vein sign and paramagnetic rim lesions can increase diagnostic specificity where appropriate MRI sequences are available.
- CSF: oligoclonal bands and/or kappa free light chains support intrathecal inflammation.
- Visual evoked potentials may show previous optic nerve demyelination, though MRI/OCT have become more central.
- OCT can show retinal nerve fibre layer thinning after optic neuritis.
- Blood tests to exclude mimics: FBC, U&E, LFT, calcium, glucose/HbA1c, ESR/CRP, TFT, B12, folate, HIV, syphilis serology, ANA/ENA/ANCA as indicated, ACE if sarcoid suspected.
- AQP4-IgG and MOG-IgG if optic neuritis, myelitis or imaging features suggest NMOSD/MOGAD.
🚩 Red Flags Against Typical MS
- Fever, meningism or encephalopathy.
- Longitudinally extensive transverse myelitis over ≥3 vertebral segments.
- Bilateral severe optic neuritis or poor recovery.
- Prominent systemic features: rash, arthritis, uveitis, pulmonary disease, weight loss.
- Peripheral neuropathy, fasciculations or lower motor neurone signs.
- Very abrupt vascular onset or purely vascular-territory lesions.
- Progressive symptoms from onset with no supportive MRI/CSF evidence.
- Consider mimics: NMOSD, MOGAD, sarcoidosis, vasculitis, B12/copper deficiency, HIV, syphilis, Lyme disease, malignancy and genetic leukodystrophies.
📊 EDSS — Expanded Disability Status Scale
The EDSS is a commonly used scale for disability in MS. It is heavily weighted toward walking ability at higher scores, but it is useful for describing disease burden, clinical trials and treatment eligibility.
| EDSS score | Meaning |
|---|---|
| 0 | Normal neurological examination. |
| 1.0–1.5 | No disability but minimal signs in one or more functional systems. |
| 2.0–2.5 | Minimal disability. |
| 3.0–3.5 | Moderate disability, but fully ambulatory. |
| 4.0–4.5 | Significant disability but able to walk without aid for about 300–500 m. |
| 5.0–5.5 | Increasing limitation in daily activities; walking distance reduced. |
| 6.0 | Requires unilateral walking aid, such as a stick or crutch. |
| 6.5 | Requires bilateral walking aids. |
| 7.0–7.5 | Essentially wheelchair-dependent. |
| 8.0–8.5 | Restricted to bed/chair for much of the day; retains some self-care function. |
| 9.0–9.5 | Bedbound and highly dependent. |
| 10 | Death due to MS. |
💊 Management of Acute Relapse
- First exclude pseudo-relapse: infection, fever, heat, metabolic disturbance, medication effects or stress.
- Treat relapse if symptoms are functionally significant or distressing.
- High-dose methylprednisolone is used to speed recovery:
- Common UK regimen: oral methylprednisolone 500 mg daily for 5 days, or
- IV methylprednisolone 1 g daily for 3–5 days if oral therapy is unsuitable or admission is required.
- Steroids improve speed of recovery but do not clearly alter long-term disability.
- Consider gastric protection, glucose monitoring, mood/psychosis risk, infection risk and osteoporosis risk where relevant.
- Plasma exchange should be considered for severe acute relapses that are steroid-resistant, especially severe optic neuritis, myelitis or brainstem relapse.
🧬 Disease-Modifying Therapy
- DMT choice depends on disease activity, relapse severity, MRI activity, pregnancy plans, comorbidities, infection risk and patient preference.
- Moderate-efficacy options include interferon beta, glatiramer acetate, dimethyl fumarate and teriflunomide.
- Higher-efficacy options include natalizumab, ocrelizumab, ofatumumab, alemtuzumab, cladribine, fingolimod and other S1P modulators depending on local/NICE eligibility.
- Progressive MS treatment is specialist-led; ocrelizumab and siponimod may be relevant in selected patients depending on phenotype and inflammatory activity.
- Monitor for treatment-specific risks, including PML, lymphopenia, infections, malignancy risk, liver injury and pregnancy-related issues.
🧬 Multiple Sclerosis — Disease-Modifying Therapies
💡 Disease-modifying therapies (DMTs) reduce relapse frequency, MRI activity and disability accumulation in selected patients with MS. They are not used for acute relapse treatment; acute disabling relapses are usually treated with high-dose methylprednisolone, with plasma exchange considered for severe steroid-resistant relapses.
| Drug / class | Typical indication | Important adverse effects / cautions |
|---|---|---|
| Beta interferons
interferon beta-1a / beta-1b / peginterferon |
|
|
| Glatiramer acetate |
|
|
| Teriflunomide |
|
|
| Dimethyl fumarate |
|
|
| S1P receptor modulators
fingolimod, ponesimod, ozanimod, siponimod |
|
|
| Cladribine |
|
|
| Natalizumab |
|
|
| Ocrelizumab |
|
|
| Ofatumumab |
|
|
| Alemtuzumab |
|
|
| Autologous haematopoietic stem cell transplantation
AHSCT |
|
|
🧠 Practical Pearls
- Lower/moderate activity: interferons, glatiramer, teriflunomide or dimethyl fumarate may be considered.
- Highly active relapsing MS: natalizumab, ocrelizumab, ofatumumab, cladribine, alemtuzumab or S1P modulators may be considered depending on criteria.
- JCV-positive/high-index: natalizumab carries higher PML risk; alternatives such as anti-CD20 therapy or cladribine may be preferred.
- Pregnancy planning: discuss early with MS specialist team; some DMTs are contraindicated or need washout.
- Before immunosuppressive DMT: check vaccination status, infection screening, baseline FBC/LFTs and drug-specific monitoring requirements.
⚖️ Symptom Management
- Fatigue: energy conservation, exercise programmes, sleep optimisation; amantadine may be considered.
- Spasticity: physiotherapy, stretching, baclofen, gabapentin, tizanidine, benzodiazepines or botulinum toxin in selected cases.
- Neuropathic pain: amitriptyline, duloxetine, gabapentin or pregabalin depending on comorbidity and tolerability.
- Bladder dysfunction: exclude UTI; antimuscarinics, mirabegron, intermittent self-catheterisation or urology referral as appropriate.
- Oscillopsia/nystagmus: gabapentin or memantine may help selected patients.
- Mood/cognition: screen for depression, anxiety and cognitive impairment; involve neuropsychology/rehabilitation where available.
- Mobility: physiotherapy, occupational therapy, falls assessment, FES, walking aids and spasticity management.
📉 Prognosis
- Better prognosis: younger onset, female sex, optic neuritis or sensory onset, complete recovery from early relapses, low early lesion burden.
- Worse prognosis: male sex, older onset, progressive onset, early motor/cerebellar involvement, poor relapse recovery, high MRI lesion burden, spinal cord involvement and early disability accumulation.
Cases - Multiple Sclerosis (MS)
- Case 1 - Optic Neuritis 👁️:
A 27-year-old woman presents with subacute painful loss of vision in her right eye, worse with eye movement. Examination shows reduced visual acuity, reduced colour vision, central scotoma and relative afferent pupillary defect.
Diagnosis: Optic neuritis due to inflammatory demyelination.
Management: MRI brain/spine/orbits, AQP4/MOG testing if atypical, consider high-dose methylprednisolone if functionally significant, and neurology review for MS risk and DMT planning. - Case 2 - Cervical Cord Relapse with Lhermitte’s Sign ⚡:
A 32-year-old man develops leg stiffness, urinary urgency and electric-shock sensations down the spine when flexing his neck. Examination shows spastic paraparesis, brisk reflexes and a sensory level.
Diagnosis: Demyelinating myelitis with Lhermitte’s sign.
Management: MRI spine/brain, exclude mimics including B12 deficiency, syphilis, HIV, AQP4/MOG disease; treat significant relapse with high-dose steroids. - Case 3 - Brainstem Involvement 🎯:
A 29-year-old woman complains of double vision and vertigo. Examination shows internuclear ophthalmoplegia, with impaired adduction of one eye and abducting nystagmus of the other. MRI shows periventricular and infratentorial lesions.
Diagnosis: MS brainstem relapse.
Management: Steroids if disabling, MRI/CSF to support diagnosis, and DMT initiation if MS confirmed. - Case 4 - Progressive MS ⏳:
A 45-year-old man develops gradually worsening gait stiffness and bladder urgency over 2 years, without clear relapses. Examination shows spastic paraparesis and a broad-based gait.
Diagnosis: Progressive MS phenotype if supported by MRI/CSF and mimics excluded.
Management: Specialist MS review, rehabilitation, spasticity/bladder management, falls prevention and consideration of DMT if criteria met.
Teaching Commentary 🧠
MS is a chronic inflammatory demyelinating disease of the CNS, commonly affecting young adults and more often women. Classic presentations include optic neuritis, partial myelitis, brainstem syndromes such as internuclear ophthalmoplegia, sensory relapses, cerebellar symptoms and progressive spastic paraparesis. Modern diagnosis relies on typical clinical syndromes plus MRI/CSF biomarkers, with updated criteria recognising the optic nerve, central vein sign, paramagnetic rim lesions and CSF biomarkers such as oligoclonal bands or kappa free light chains. Do not diagnose MS without excluding mimics: check for alternative inflammatory, infectious, metabolic and vascular causes, including syphilis, HIV, B12 deficiency, AQP4-NMOSD and MOGAD where appropriate. Acute disabling relapses are treated with high-dose methylprednisolone; plasma exchange is an important escalation option for severe steroid-resistant relapses.
📚 References
- McDonald criteria 2024 revisions: Diagnosis of multiple sclerosis: 2024 revisions of the McDonald criteria.
- NICE: Multiple sclerosis in adults: management.
- NICE technology appraisals for disease-modifying therapies in MS.
- ECTRIMS: Diagnosis of MS — 2024 revisions of the McDonald criteria.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery