Related Subjects:
|Assessing Chest Pain
|Acute Coronary Syndrome (ACS) General
|Aortic Dissection
|Pulmonary Embolism
|Acute Pericarditis
|Diffuse Oesophageal Spasm
|Gastro-oesophageal reflux
|Oesophageal Perforation Rupture
|Pericardial Effusion Tamponade
|Pneumothorax
|Tension Pneumothorax
|Shingles
| Ankle-Brachial pressure Index (ABPI) and Peripheral Vascular Disease
| Peripheral Arterial Disease (PAD)
| Abdominal Aortic Aneurysm (AAA)
| Carotid Endarterectomy
| Buerger's disease (Thromboangiitis obliterans )
| Leriche syndrome (aortoiliac occlusive disease)
🚨 Aortic Dissection is a life-threatening emergency caused by a tear in the aortic intima, allowing blood to enter the media and create a false lumen. Early recognition is critical: misdiagnosis as MI ❤️🔥 or PE 🩸 is dangerous, as anticoagulation can worsen outcomes. Urgent imaging and specialist referral are essential.
| 🩺 Management of Acute Aortic Dissection |
- 🚨 Immediate Stabilisation (ABC):
Airway, Breathing, Circulation 💨❤️. Ensure high-flow oxygen, establish ≥2 large-bore IV lines, monitor vital signs, continuous ECG and pulse oximetry.
- 🔍 Diagnostics:
Urgent imaging is essential. First choice: CT Aortogram (contrast-enhanced). Alternative if unstable: Transoesophageal echocardiography (TOE). Assess for extension, branch vessel involvement, and pericardial effusion.
- 💔 Type A Dissection (Ascending Aorta):
Immediate cardiothoracic referral 🚑. Patient requires urgent surgical repair. Delay increases mortality 1–2% per hour.
- 🩹 Pain Management:
IV opioids (morphine 2.5–5 mg titrated) for severe pain; reduces sympathetic stimulation and blood pressure surges.
- 💊 Blood Pressure & Heart Rate Control:
Goal: reduce shear stress (dp/dt) ⬇️. First-line: IV Labetalol 20 mg increments (beta-blockade, HR target ~60 bpm). Second-line/adjunct: Nitroprusside if BP remains elevated after beta-blockade.
- ⚠️ What to Avoid:
Anticoagulants, antiplatelets, and thrombolytics ❌ before dissection is excluded. These significantly increase risk of fatal haemorrhage.
- 📌 Supportive Measures:
Continuous telemetry, urinary catheter for monitoring output, prepare for potential cardiothoracic ICU transfer, correct electrolyte imbalances, and monitor end-organ perfusion.
- 🩺 Type B Dissection (Descending Aorta):
Uncomplicated: medical management with strict blood pressure control and analgesia. Complicated: consider endovascular repair (TEVAR).
|
📖 Overview
- Mortality: ~40% die before reaching hospital ⚰️; an additional 10% peri/post-op.
- High-risk features: severe sudden chest/back pain, BP differences, syncope, neurologic deficits.
- Types: Stanford A (ascending aorta) and B (descending aorta), guiding management.
- NICE and ESC guidelines emphasise rapid recognition, blood pressure control, imaging, and cardiothoracic referral.
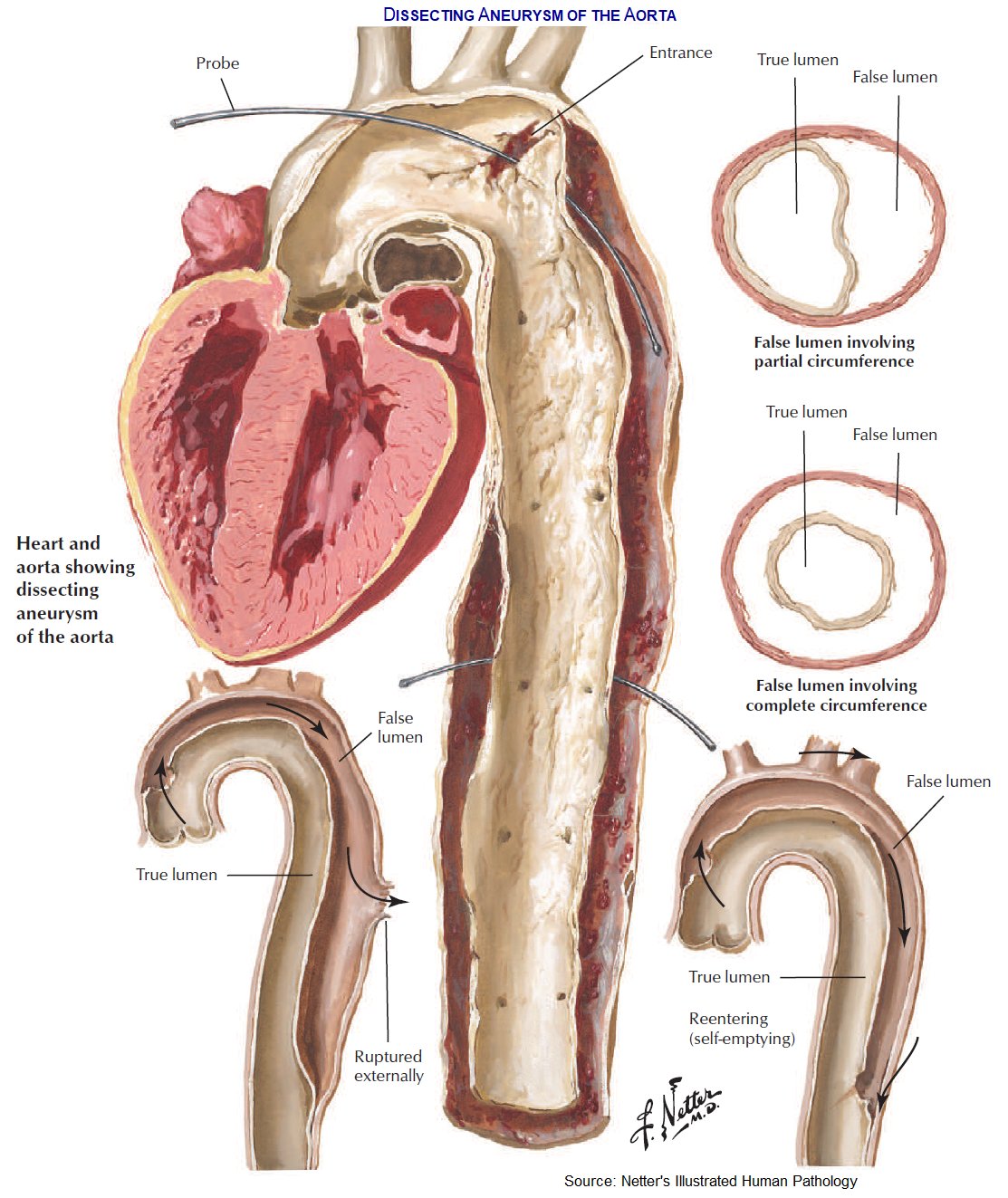
🧬 Pathophysiology
- The aortic wall has three layers: intima, media, adventitia.
- A tear in the intima allows blood under high pressure to dissect into the media → formation of a false lumen.
- Complications: rupture, tamponade, branch vessel obstruction, acute aortic regurgitation, MI, stroke.
- Extension can be antegrade (distal vessels) or retrograde (aortic valve/coronaries).
- Shear stress and hypertension exacerbate propagation; connective tissue disorders weaken the media.
🌍 Epidemiology
- Incidence: ~3–4 per 100,000/year; more common in males ♂, age >60.
- Type A: ~2/3 of cases; Type B: ~1/3.
- Risk factors: chronic hypertension, connective tissue disease (Marfan, Ehlers–Danlos), bicuspid aortic valve, pregnancy (3rd trimester), cocaine, trauma, aortitis.
- Mortality rises 1–2% per hour if Type A dissection is untreated.
🧬 Causes / Risk Factors
| Category | Examples / Details |
|---|
| Hypertension | Chronic uncontrolled hypertension in elderly patients; most common predisposing factor |
| Connective tissue disorders | Marfan, Ehlers–Danlos, Loeys–Dietz → medial cystic degeneration |
| Aortitis / Vasculitis | Takayasu arteritis, Giant Cell Arteritis, syphilitic aortitis |
| Congenital / Structural | Bicuspid aortic valve, coarctation, post-surgical aorta repair |
| Trauma / Iatrogenic | Blunt chest trauma, catheterisation, aortic surgery |
| Drugs / Toxins | Cocaine, amphetamines, sympathomimetics (↑ shear stress) |
| Pregnancy / Peripartum | 3rd trimester or early postpartum due to hormonal and haemodynamic changes |
🫀 Classification of Thoracic Aortic Dissection
🧠 Core idea: thoracic aortic dissection is classified mainly by whether the ascending aorta is involved.
This matters because ascending aortic involvement has a high risk of tamponade, acute aortic regurgitation, coronary occlusion, stroke and rupture, so it usually needs urgent surgery.
| Classification |
Type |
Anatomy |
Typical management |
Stanford classification
Most clinically useful |
A |
Involves the ascending aorta, regardless of where the tear starts or how far it extends.
|
🚨 Surgical emergency
Urgent cardiothoracic surgery + BP/HR control while awaiting operation.
|
| B |
Does not involve the ascending aorta. Usually starts distal to the left subclavian artery in the descending thoracic aorta.
|
💊 Usually medical management initially: IV beta-blocker, BP control, analgesia.
Endovascular/surgical repair if complicated.
|
DeBakey classification
More anatomical detail |
I |
Starts in the ascending aorta and extends into the arch and often descending aorta.
|
Equivalent to Stanford A → urgent surgery.
|
| II |
Confined to the ascending aorta.
|
Equivalent to Stanford A → urgent surgery.
|
| III |
Starts in the descending aorta, distal to the left subclavian artery.
|
Equivalent to Stanford B → usually medical unless complicated.
|
🧠 Simple Memory Aid
- 🅰️ Stanford A = Ascending aorta involved → urgent surgery.
- 🅱️ Stanford B = Beyond the left subclavian → usually medical first.
- 📍 DeBakey I and II both involve the ascending aorta, so both are Stanford A.
- 📍 DeBakey III begins in the descending aorta, so it is Stanford B.
⚠️ Complicated Type B Dissection
| Complication |
Why it matters |
| Persistent or recurrent pain |
Suggests ongoing propagation or impending rupture. |
| Uncontrolled hypertension |
Continued shear stress increases risk of extension or rupture. |
| Malperfusion |
Renal, mesenteric, spinal cord or limb ischaemia may occur if branch vessels are compromised. |
| Rupture or impending rupture |
Requires urgent endovascular or surgical intervention. |
| Rapid aortic expansion |
Higher rupture risk; usually needs specialist intervention. |
📌 Learning tip: In exams and acute medicine, always classify dissection first as Stanford A or B.
The key question is: is the ascending aorta involved? If yes, it is Type A and the patient needs urgent cardiothoracic discussion even if they look temporarily stable.
🩺 Clinical Presentation
- Sudden severe chest/back pain: “tearing”, radiates to interscapular area ⚡🖤.
- BP asymmetry between arms >20 mmHg.
- New diastolic murmur of aortic regurgitation.
- Syncope (15%), neurological deficits, limb ischemia, abdominal pain.
- Shock or hypotension → tamponade or rupture.
- Pulsus paradoxus or absent peripheral pulses indicate major compromise.
❗ Complications
- Type A: cardiac tamponade, aortic regurgitation, MI, stroke, rupture, death 💥
- Type B: renal or mesenteric ischemia ⚠️, spinal cord ischemia 🦽, distal limb ischemia, rupture
- Chronic dissection: aneurysm formation, persistent pain, heart failure
🔎 Investigations
- Bloods: FBC, U&E, creatinine, troponin, D-dimer (helps rule out if normal).
- ECG: may mimic MI if coronary involved; usually non-specific.
- CXR: widened mediastinum, pleural effusion.
- Transthoracic echocardiography (TTE): limited, proximal ascending aorta only.
- Transoesophageal echo (TOE): bedside, rapid, sensitive for unstable patients.
- CT Aortogram (spiral CT): gold standard for diagnosis and anatomy delineation 🖥️.
- MRI: useful in chronic cases or if contrast contraindicated.
🩺 Initial Management (Acute Phase)
- ABC: oxygen, IV access, monitor vitals 💨❤️
- Pain control: IV morphine 2.5–5 mg titrated
- Blood pressure & heart rate control: IV beta-blocker (labetalol first-line), target HR ~60 bpm, systolic BP 100–120 mmHg
- Avoid anticoagulants, antiplatelets, and thrombolytics ❌
- Urgent imaging and cardiothoracic referral for Type A dissection
- Type B: medical management if uncomplicated (strict BP control, analgesia, monitoring)
🩺 Definitive Management
| Type | Management |
|---|
| Type A (ascending) |
Urgent cardiothoracic surgery: repair ± aortic root replacement, graft. Pre-op BP control. ICU post-op care. |
| Type B (descending) |
Medical: IV antihypertensives, analgesia. Endovascular stenting (TEVAR) if complications: rupture, malperfusion, persistent pain. |
💊 Pharmacological Management
- IV Beta-blockers: labetalol or esmolol (reduce shear stress, HR)
- Vasodilators: nitroprusside if BP not controlled after beta-blocker
- Analgesia: IV opioids
- Avoid anticoagulation unless otherwise indicated
- Post-op: long-term antihypertensive therapy, surveillance imaging (CTA or MRI at 3, 6, 12 months)
🧪 Monitoring & Follow-up
- Continuous telemetry in acute phase
- Serial imaging: CT or MRI to monitor false lumen, aneurysm formation
- BP & HR targets lifelong: systolic 100–120 mmHg, HR 60–70 bpm
- Patient education: avoid high-intensity isometric exercise
- Genetic counseling if connective tissue disorder suspected
📚 Guidelines & NICE Compliance
- 2014 ESC Guidelines: “Acute aortic syndromes – diagnosis, imaging, and treatment”
- NICE (NG136, NG206): recommend urgent imaging for suspected dissection, avoid anticoagulation until diagnosis, early cardiothoracic referral, BP control, and long-term follow-up
- Conservative vs surgical management based on type, comorbidities, and complications
- Emphasis on structured care: ED recognition, ICU management, MDT review
🧑⚕️ Case Examples
- Case 1 – Type A: 58M, sudden tearing chest/back pain, unequal arm BP. ECG non-diagnostic. CT confirms ascending aorta dissection. Managed with IV labetalol, urgent surgery.
- Case 2 – Type B: 70F, interscapular back pain, hypertensive, no malperfusion. CT confirms descending dissection. Managed medically with IV antihypertensives, analgesia, monitored in ICU. TEVAR reserved for complications.
- Case 3 – Complicated: 65M, Marfan’s, chest pain, syncope, left leg weakness, hypotension. CT: Type A with branch vessel compromise. Emergency surgery + ICU care.
📊 Key Teaching Points
- Always consider dissection in acute chest/back pain, especially if tearing, radiating to back, with BP asymmetry
- Do not give anticoagulants before ruling out dissection
- Type A = surgical emergency; Type B = usually medical
- CT aortogram is gold standard; TOE useful if unstable
- Rapid BP control and pain management reduce mortality
- Follow-up imaging and lifelong BP control are essential to prevent recurrence or aneurysm formation
📚 References
