Related Subjects:
|Chest drain Insertion (Thoracostomy)
|Simple Needle Aspiration for Spontaneous Pneumothorax
|Pleural tap (thoracentesis)
🫁 Simple needle aspiration is a technique used to remove air from the pleural cavity through the chest wall, without leaving a chest drain in place.
It may be used in selected patients with primary spontaneous pneumothorax, particularly when the patient is symptomatic but clinically stable.
The aim is to allow lung re-expansion while avoiding the discomfort, complications and admission often associated with chest drain insertion.
📖 About
- 🧍 Primary spontaneous pneumothorax usually occurs in patients without known underlying lung disease.
- 🫁 Air enters the pleural space, causing partial or complete lung collapse.
- 🪡 Needle aspiration removes air using a cannula, syringe, tubing and 3-way tap.
- ✅ If successful, the cannula is removed and the patient may be observed briefly before discharge with follow-up.
- ⚠️ If unsuccessful, further intervention may be needed, such as ambulatory device or chest drain depending on local pathway and patient factors.
🧠 Pathophysiology
- 🫁 The pleural space normally has negative pressure, keeping the lung expanded against the chest wall.
- 💨 In pneumothorax, air enters this space and abolishes the normal pressure gradient.
- 📉 The affected lung recoils inward because of its elastic properties.
- 🪡 Aspiration removes pleural air, helping restore negative pleural pressure and allowing the lung to re-expand.
✅ When Needle Aspiration May Be Used
- 🧍 Selected patients with primary spontaneous pneumothorax.
- 💬 Symptomatic pneumothorax, for example breathlessness or chest discomfort.
- ✅ Patient is clinically stable with no features of tension pneumothorax.
- 🏥 Appropriate monitoring, repeat chest X-ray and follow-up are available.
🚫 When Needle Aspiration Is Not Appropriate
- 🚨 Tension pneumothorax — this needs immediate emergency decompression, not slow aspiration.
- 🫁 Secondary spontaneous pneumothorax — BTS 2023 guidance has moved away from routine needle aspiration in secondary pneumothorax.
- 📉 Physiological compromise, severe breathlessness, hypoxia or haemodynamic instability.
- 🩸 Significant bleeding risk or inability to cooperate with the procedure.
- 🔁 Persistent air leak or failed aspiration requiring further pleural intervention.
Landmarks
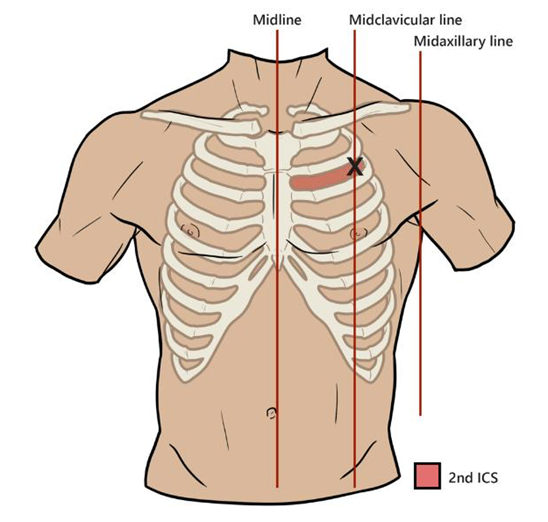
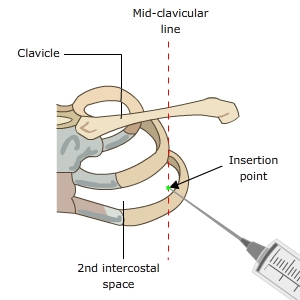
📍 Insertion Site
- 📌 Traditional site: 2nd intercostal space, mid-clavicular line.
- 🦴 Identify the sternal angle, then the 2nd rib; the space below the 2nd rib is the 2nd intercostal space.
- 🔺 Alternative site: the safe triangle, commonly used for pleural procedures and chest drain insertion.
- ⚠️ Always insert just above the upper border of the rib to avoid the neurovascular bundle running under the rib.
🔺 The Safe Triangle
| Boundary |
Anatomical landmark |
| Anterior border |
Lateral edge of pectoralis major |
| Posterior border |
Anterior edge of latissimus dorsi |
| Inferior border |
Line above the 5th intercostal space / nipple line |
| Apex |
Below the axilla |
🧰 Equipment
- 🧤 Sterile gloves, gown, antiseptic solution and sterile drapes.
- 🪡 Cannula, usually no larger than 16G; many kits use 14–16G depending on local policy.
- 💉 10 mL syringe with sterile saline for insertion and confirmation.
- 💉 50 mL syringe for aspiration.
- 🔄 3-way tap and short connecting tubing.
- 🩹 Occlusive dressing.
- 🩻 Access to repeat chest X-ray after the procedure.
🩺 Method
- 🗣️ Explain the procedure, risks and alternatives, then obtain consent where possible.
- 🛏️ Position the patient slightly reclined, with monitoring and oxygen if required.
- 📍 Identify and mark the insertion site.
- 🧼 Use aseptic technique: clean the skin and apply sterile drapes.
- 💉 Infiltrate local anaesthetic, usually 1% lidocaine, down to the pleura.
- 🪡 Insert the cannula through the chest wall in a controlled horizontal plane.
- 💨 Aspiration of air confirms entry into the pleural space.
- 🧷 Remove the needle/trocar, leaving the cannula in place.
- 🔄 Attach the cannula to short tubing, a 3-way tap and a 50 mL syringe.
- 💨 Aspirate 50 mL of air, turn the tap, and expel the air into the atmosphere.
- 🔁 Repeat aspiration until no more air is obtained, the patient coughs, or approximately 2.5 L has been aspirated.
- 🩻 Repeat chest X-ray to assess lung re-expansion.
- ✅ If successful, remove the cannula and apply an occlusive dressing.
- ➡️ If unsuccessful, follow the local pneumothorax pathway; this may involve ambulatory device or chest drain insertion.
📊 Outcome
- ✅ Initial success in primary spontaneous pneumothorax is often around 60–70%.
- 🏠 Successful aspiration increases the chance of discharge compared with chest drain insertion.
- ⚠️ Complication rates are generally lower than with chest drain insertion.
- 🔁 Recurrence rates are broadly similar to chest drain management at short-term and 1-year follow-up.
- 🕒 After successful aspiration, patients usually need a short period of observation and clear follow-up advice.
⚠️ Complications
- ❌ Failed aspiration or early recurrence.
- 💨 Persistent air leak.
- 🩸 Bleeding or intercostal vessel injury.
- 🦠 Infection, although uncommon with aseptic technique.
- 🫁 Re-expansion pulmonary oedema, rare but potentially serious after rapid re-expansion.
- 😰 Pain, vasovagal symptoms or anxiety during the procedure.
🧠 Practical Tips
- 👥 Use two people where possible: one to stabilise the cannula and operate the 3-way tap, the other to aspirate.
- 🔗 Always attach a short connecting tube; direct syringe attachment increases the risk of cannula kinking or accidental dislodgement.
- 🔄 Be careful with the 3-way tap — turning it the wrong way can push air back into the pleural space.
- 💪 Aspiration can be slow and tiring; 2.5 L requires up to 50 full 50 mL syringe aspirations.
- 🔥 The syringe may become warm due to repeated friction.
- 🩻 Always repeat imaging after aspiration before deciding on discharge or escalation.
🚨 Tension Pneumothorax — Do Not Delay
🚨 Tension pneumothorax is a clinical emergency.
If the patient has severe respiratory distress, hypotension, tracheal deviation, raised JVP or cardiovascular collapse, do not wait for a chest X-ray.
Immediate decompression is required, followed by definitive pleural drainage.
🏥 UK Guideline Context
- 🇬🇧 BTS 2023 guidance uses a more symptom-based approach rather than relying only on pneumothorax size.
- ✅ Conservative management may be considered for asymptomatic or minimally symptomatic primary spontaneous pneumothorax in stable adults.
- 🪡 Needle aspiration remains an option for selected symptomatic primary spontaneous pneumothorax.
- 🫁 Secondary spontaneous pneumothorax usually requires closer inpatient management and often chest drain treatment rather than simple aspiration.
💡 Exam Tip
🧠 Primary spontaneous pneumothorax: consider conservative care, ambulatory management, needle aspiration or chest drain depending on symptoms, stability and local pathway.
🫁 Secondary spontaneous pneumothorax: lower physiological reserve, higher risk, and usually needs admission and respiratory input.
🚨 Tension pneumothorax: diagnose clinically and decompress immediately.
References
