
🦠 Coronavirus SARS-CoV-2 (COVID-19): Management is largely supportive for mild disease. NICE guidance recommends specific therapies such as corticosteroids only in patients requiring supplemental oxygen or with severe/critical illness.
📖 About
- COVID-19 is caused by SARS-CoV-2, a novel coronavirus first identified in late 2019.
- Transmission: respiratory droplets, aerosols, and fomites; high human-to-human transmissibility.
🌍 Origin
- First identified in Wuhan, China, December 2019; linked to live animal markets.
🔬 Virology & Aetiology
- SARS-CoV-2 structural proteins:
- Spike (S) 🗝️ – binds ACE2 receptors in lungs, GI tract, kidneys, and brain.
- Envelope (E) 📦 – assembly and release of viral particles.
- Matrix (M) 🧱 – structural integrity.
- Nucleocapsid (N) 🧬 – protects viral RNA.
- Primary pathology: viral pneumonia. Mortality ~1% overall; higher in elderly or comorbid patients.
🧫 Pathophysiology
- Diffuse alveolar damage: hyaline membranes, pneumocyte desquamation, mononuclear infiltrates, fibroblastic proliferation.
- ACE2 receptor expression beyond lungs explains multi-organ involvement (kidneys, heart, liver, brain).
⚠️ High-Risk Groups
- Older adults, care home residents.
- Comorbidities: diabetes, obesity, hypertension, chronic lung disease, cardiovascular disease, cancer, immunosuppression.
- Higher risk in certain ethnic groups (South Asian, Afro-Caribbean).
- Other factors under study: vitamin D deficiency, immune variation.
🩺 Clinical Features
- Incubation: 2–14 days (median 5 days).
- Common: fever 🌡️, dry cough, dyspnoea, fatigue, myalgia, headache, confusion.
- Less common: sore throat, rhinorrhoea, chest pain, diarrhoea, nausea/vomiting.
- Complications: viral pneumonia → type 1 respiratory failure, myocarditis ❤️, acute kidney injury 🧽, thromboembolism 🩸.
📊 Severity Classification (NICE)
- Asymptomatic: PCR+ but no symptoms.
- Mild: fever/cough, no hypoxia.
- Moderate: lower respiratory disease, SpO₂ ≥94% on room air.
- Severe: RR >30, SpO₂ <94%, PaO₂/FiO₂ <300, >50% lung infiltrates.
- Critical: respiratory failure, septic shock, multi-organ dysfunction.
🚑 Complications
- Cytokine Storm 🌪️ – hyperinflammatory response → ARDS, shock.
- Cardiac ❤️ – myocarditis, arrhythmias, ACS-like syndromes.
- Renal/Liver 🧽 – AKI, liver enzyme derangement; 10–15% of critical patients may need renal replacement therapy.
- Thromboembolic 🩸 – pulmonary embolism, DVT; prophylactic anticoagulation recommended in hospitalised patients.
🔍 Investigations (NICE-compliant)
- Bloods: lymphopenia, ↑ CRP, ↑ D-dimer, ± deranged LFTs/renal function.
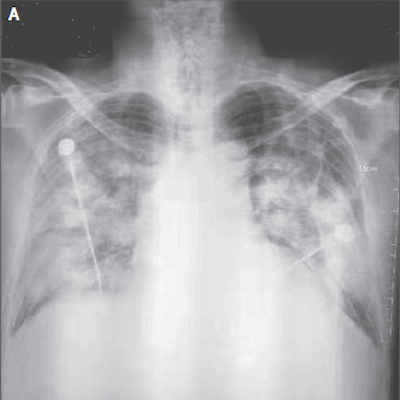
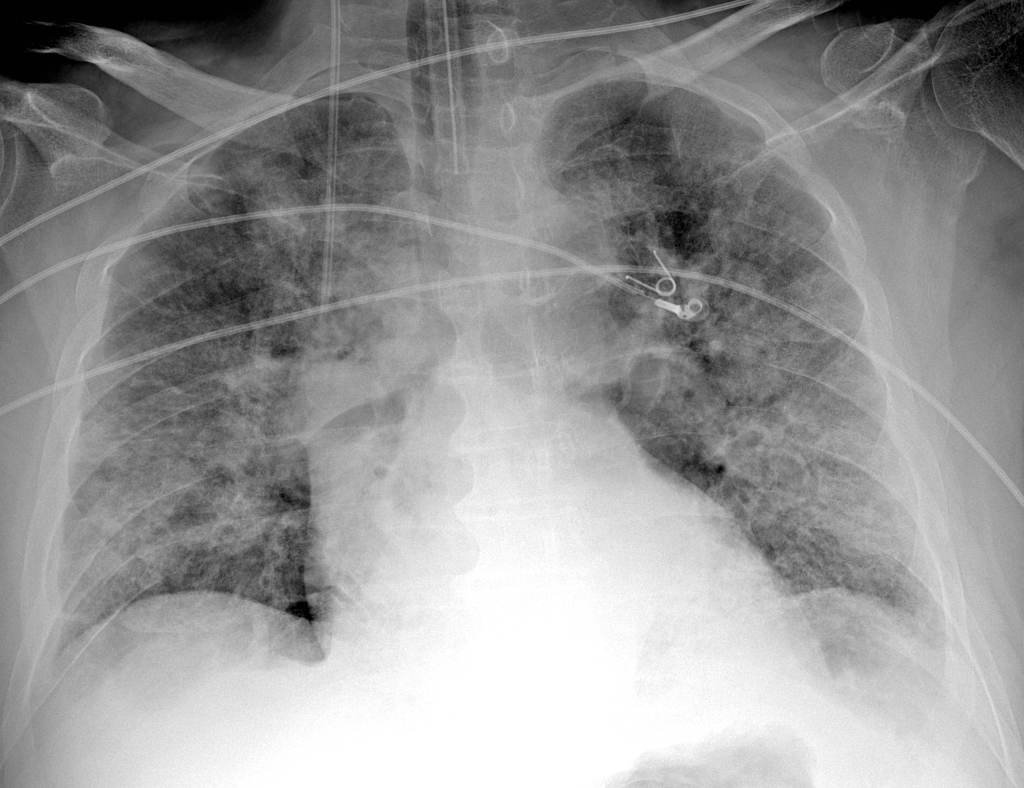
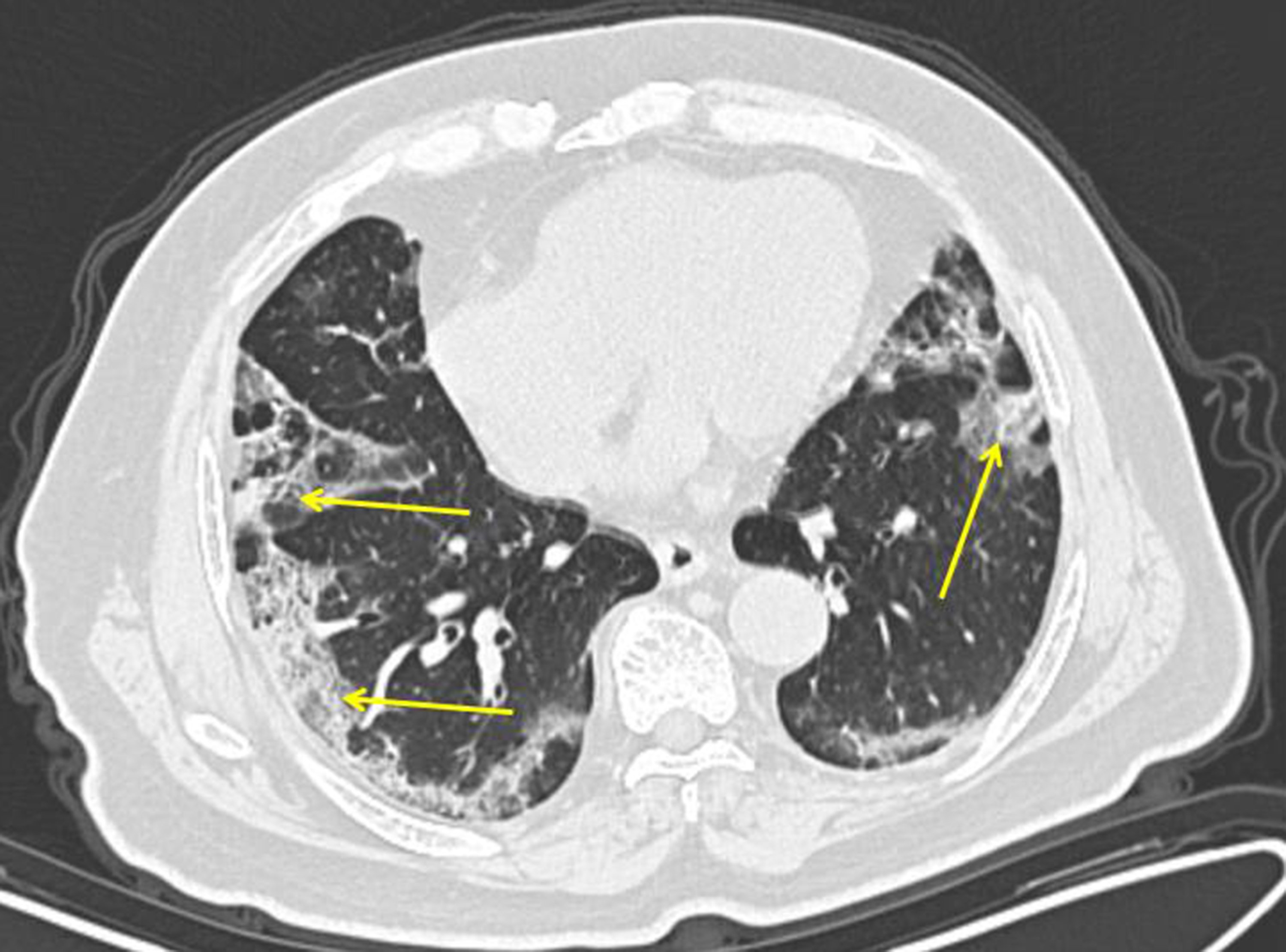
- Imaging: CXR: bilateral patchy opacities; CT: ground-glass changes; CTPA if PE suspected.
- Microbiology: RT-PCR nasal/throat swabs; antibody testing for past exposure.
- Cardiac markers: ↑ troponin/BNP if myocardial involvement suspected.
🛡️ Prevention (NICE CKS 2025)
- 😷 Face masks, hand hygiene 🤲, social distancing ↔️.
- Isolation of confirmed/suspected cases; contact tracing.
- PPE for healthcare workers; environmental cleaning and aseptic techniques.
- Vaccination: COVID-19 vaccines as per national immunisation schedule.
💊 Management (NICE CKS 2025)
- Mild disease: supportive care at home – fluids, rest, antipyretics (paracetamol), monitoring symptoms.
- Moderate/severe disease: hospital admission, supplemental oxygen (target SpO₂ 92–96%), monitor for deterioration.
- Corticosteroids: dexamethasone 6 mg OD up to 10 days for patients requiring oxygen or ventilatory support.
- Antivirals: remdesivir may be used in selected severe cases per local protocols; not for routine mild disease.
- Respiratory support: HFNO or NIV for hypoxia; mechanical ventilation in ICU for ARDS (low tidal volume + prone positioning).
- Thromboprophylaxis 🩸: LMWH in hospitalised patients unless contraindicated.
- Other supportive care: treat bacterial superinfection, fluid balance, monitor multi-organ function.
Cases - COVID-19
- Case 1 - Mild Illness: 28-year-old, fever, anosmia, dry cough. SpO₂ 98% RA. PCR+. Management: home isolation, fluids, paracetamol, monitoring.
- Case 2 - Moderate Pneumonia: 54-year-old with diabetes, SpO₂ 91% RA, RR 28, CXR bilateral infiltrates. Management: admit, controlled O₂ 92–96%, dexamethasone, prophylactic LMWH, antibiotics only if bacterial superinfection suspected.
- Case 3 - Severe Disease with ARDS: 66-year-old, SpO₂ 82%, RR 36, diffuse GGO on CXR. Management: escalate to ICU, CPAP/NIV, consider intubation, dexamethasone ± tocilizumab, prone positioning, careful fluid management.
- Case 4 - Post-COVID PE: 49-year-old, dyspnoea, segmental PE on CTPA. Management: anticoagulation (LMWH/DOAC), O₂ therapy, monitor for extended anticoagulation, rehabilitation support.
Teaching Commentary 🧠
COVID-19 spectrum: mild → moderate → severe/critical with multi-organ involvement. Key NICE principles: supportive care, oxygen targeting, dexamethasone for hypoxic patients, thromboprophylaxis in hospitalised cases, early ICU referral for ARDS. Monitor vulnerable groups (elderly, comorbidities) closely, especially around days 7–10 when deterioration is common.
