
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
ECG - Sinoatrial block ❤️
Related Subjects: |ECG Basics |ECG Axis |ECG Analysis |ECG LAD |ECG RAD |ECG Low voltage |ECG Pathological Q waves |ECG ST/T wave changes |ECG LBBB |ECG RBBB |ECG short PR |ECG Heart Block |ECG Asystole and P wave asystole |ECG QRS complex |ECG ST segment |ECG: QT interval |ECG: LVH |ECG RVH |ECG: Bundle branch blocks |ECG Dominant R wave in V1 |ECG Acute Coronary Syndrome |ECG Sino atrial block
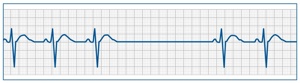
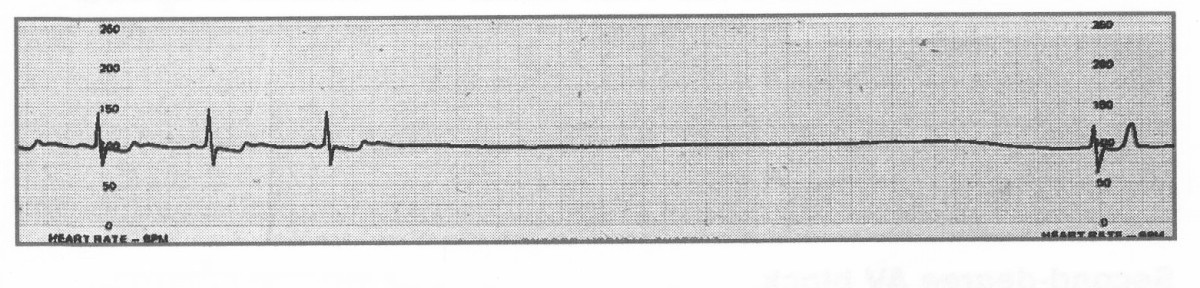
Sinoatrial (SA) block occurs when impulses from the SA node are delayed or fail to reach the atria. This leads to intermittent pauses in atrial and ventricular activity. Causes include high vagal tone (e.g., in athletes or during sleep), medications that depress conduction, or intrinsic SA node disease. Continuous monitoring (e.g., 24-hour Holter) may be needed for diagnosis, particularly in patients with infrequent symptoms. Pauses >3 seconds, especially if associated with syncope, dizziness, or fatigue, often prompt consideration for a pacemaker. ⚡
🫀 About Sinoatrial Block
- Definition: Failure or delay of impulse conduction from the SA node to atria.
- Mechanism:
- Failure of impulse initiation (intrinsic node dysfunction).
- Impulse generation occurs but is blocked before reaching the atria.
📌 Aetiology
- Increased Vagal Tone: Common in young athletes, during sleep, or in vasovagal episodes.
- Medications: Beta-blockers, calcium channel blockers, digoxin, amiodarone.
- Intrinsic SA Node Disease: Age-related fibrosis, sick sinus syndrome.
- Other Causes: Myocarditis, ischaemic heart disease, electrolyte imbalance (esp. hyperkalemia), thyroid dysfunction.
📊 Types of Sinoatrial Block
- First-Degree: Delay in conduction, invisible on ECG, asymptomatic.
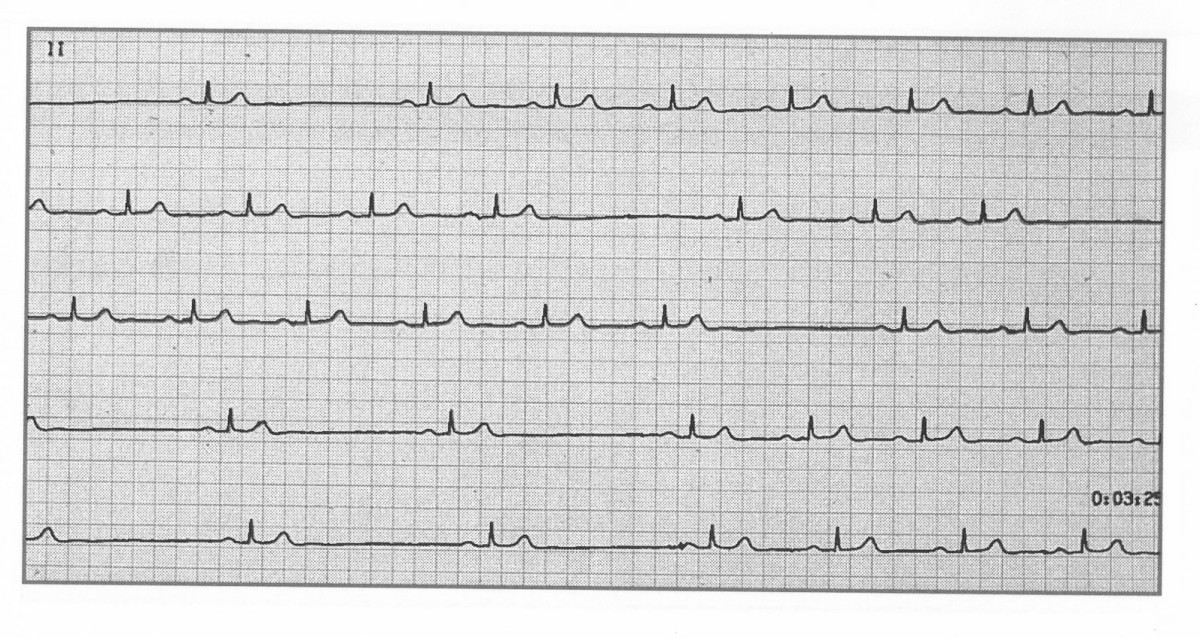
- Second-Degree: Intermittent failure of conduction → dropped beats.
- Type I (Wenckebach): Progressive delay then dropped beat (rare, difficult to see).
- Type II: Random dropped beats without progressive delay → more serious, risk of progression.
- Third-Degree (Complete): No impulses conducted → complete pause, may require escape rhythm.
💡 Exam Tip: Differentiate SA block from sinus arrest – in SA block, the pause is an exact multiple of the normal P-P interval; in sinus arrest, it is not.
🩺 Clinical Features
- Symptoms: Dizziness, presyncope, fatigue, palpitations, syncope (if long pauses).
- Signs: Bradycardia, irregular pauses on auscultation or telemetry.
🔎 Investigations
- 24-Hour Holter / Event Recorder: For intermittent blocks.
- Electrolytes: Look for hyperkalemia, magnesium/calcium disturbances.
- Thyroid Function: Both hypo- and hyperthyroidism can precipitate bradyarrhythmia.
- Echocardiography: If structural disease is suspected.
⚕️ Management
- Review and withdraw offending drugs if possible.
- Correct reversible causes (electrolytes, thyroid, myocarditis).
- Pacemaker: Indicated for symptomatic patients (e.g., syncope, presyncope, heart failure) or if pauses >3 seconds, in line with ESC/NICE pacing guidelines.
🚨 Key Clinical Pearl: Symptomatic SA block is considered part of the "sick sinus syndrome" spectrum and usually requires pacing. Asymptomatic pauses <3 seconds may not need intervention.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery