Related Subjects:
|Cystic Fibrosis
|Sweat Test
|Osteoporosis
|Malabsorption
|Bronchiectasis
|Pseudomonas infection (Pseudomonas aeruginosa)
|Autosomal Recessive
|Genetic Mutations
|Clustered Regularly Interspaced Short Palindromic Repeats CRISPR
⚠️ Cystic Fibrosis (CF) is an autosomal recessive CFTR channel disorder causing
impaired chloride transport → dehydrated secretions → impaired mucociliary clearance → chronic infection and inflammation.
✅ Diagnosis is based on clinical features and/or newborn screening plus evidence of CFTR dysfunction (for example, sweat chloride testing and genetic testing).
💡 With modern specialist care and CFTR modulators, median predicted survival in the UK now exceeds 50 years.
📖 About
- Inherited defect of the Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) protein.
- Leads to abnormal salt and water transport across epithelial surfaces.
- Results in dehydrated, tenacious secretions causing airway obstruction, chronic infection, inflammation, and multisystem disease.
- Commonly affects the respiratory, gastrointestinal, endocrine, hepatobiliary, reproductive, and musculoskeletal systems.
🧬 Aetiology
- Autosomal recessive inheritance.
- CFTR gene is on chromosome 7q31.2.
- More than 2,000 CFTR variants have been described.
- F508del (ΔF508) is the most common pathogenic variant in the UK population.
- Genotype does not fully predict severity because phenotype is influenced by modifier genes, environment, infection burden, and treatment access.
- Incidence in the UK is approximately 1 in 2,500 live births; carrier frequency is around 1 in 25 in people of Northern European ancestry.
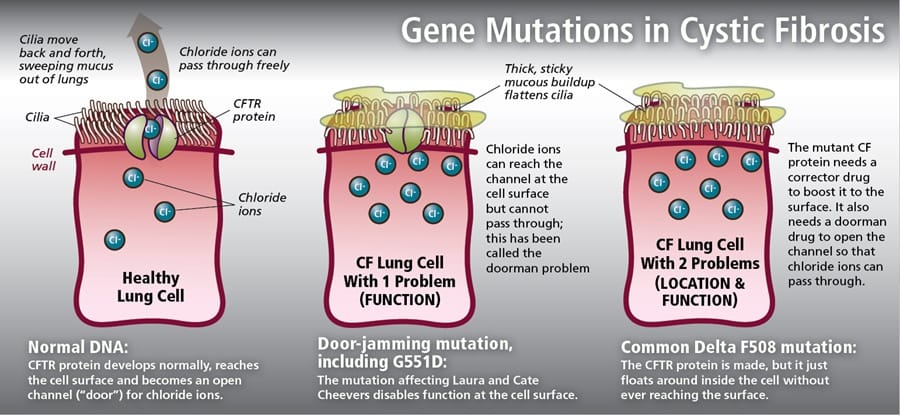
🧪 Gene Mutations & Effects
🔍 Diagnosis
- Often detected by newborn screening using raised immunoreactive trypsinogen (IRT), followed by confirmatory testing.
- Diagnosis is supported by clinical manifestations together with evidence of CFTR dysfunction.
- Sweat chloride ≥60 mmol/L is consistent with CF in the appropriate clinical context.
- 30–59 mmol/L is intermediate / borderline and needs further assessment.
- Genetic testing may identify 2 CF-causing CFTR variants.
- Additional physiological testing such as nasal potential difference or intestinal current measurement may be used in atypical or inconclusive cases.
🧪 Investigations
- Sweat chloride test: key diagnostic test; usually repeated or interpreted alongside genetics and clinical features.
- Genetic testing: mutation analysis helps confirm diagnosis and identify eligibility for CFTR modulator therapy.
- Pancreatic function: faecal elastase for pancreatic insufficiency.
- Respiratory assessment: spirometry, sputum or cough swab microbiology, chest imaging if indicated.
- Microbiology: monitor for Pseudomonas aeruginosa, Staphylococcus aureus, Haemophilus influenzae, and other pathogens.
- Endocrine screening: screen annually for CF-related diabetes; in children this is commonly with OGTT from age 10 years.
- Nutritional assessment: growth, BMI, fat-soluble vitamin status.
- Hepatobiliary review: LFTs and assessment for liver disease if indicated.
- Fertility assessment: semen analysis in adult males if needed; consider reproductive counselling.
🫁 Clinical Features (Respiratory)
- Persistent or recurrent cough.
- Recurrent chest infections.
- Wheeze and progressive airflow obstruction.
- Bronchiectasis due to chronic infection-inflammation cycles.
- Pseudomonas colonisation is associated with worse long-term lung outcomes.
- Chronic rhinosinusitis and nasal polyps are common.
- Complications include massive haemoptysis, pneumothorax, and respiratory failure.
🍽️ Clinical Features (Gastrointestinal / Nutritional)
- Meconium ileus in neonates.
- Pancreatic insufficiency causing malabsorption, steatorrhoea, abdominal distension, and failure to thrive.
- Distal intestinal obstruction syndrome (DIOS).
- Poor weight gain and fat-soluble vitamin deficiency.
- Hepatic steatosis, focal biliary cirrhosis, gallstones, and chronic liver disease may occur.
- CF-related diabetes (CFRD) becomes increasingly common with age.
🧍 Other System Features
- Clubbing.
- Low bone mineral density / osteoporosis.
- Arthropathy may occur.
- Male infertility is common, usually due to congenital bilateral absence of the vas deferens.
- Females may have reduced fertility, but many can conceive.
- Salty-tasting sweat is a classic clue.
📊 Summary of Testing
| Diagnostic Test |
Description |
Interpretation |
| 🧪 Sweat Chloride Test |
Measures sweat chloride after pilocarpine iontophoresis |
≥60 mmol/L supports CF; 30–59 mmol/L intermediate; <30 mmol/L usually makes CF unlikely |
| 🧬 Genetic Testing |
Identifies CFTR variants |
2 disease-causing variants support diagnosis |
| ⚡ Nasal Potential Difference |
Assesses CFTR-dependent ion transport |
Useful in atypical or indeterminate cases |
| 👶 Newborn IRT |
Screening blood spot test |
Raised result triggers confirmatory testing |
⚠️ Complications
- Chronic suppurative lung disease and bronchiectasis.
- Respiratory failure and need for transplant assessment in advanced disease.
- CFRD.
- Low bone mineral density / osteoporosis.
- Chronic liver disease and portal hypertension.
- Reduced fertility or infertility.
- Psychological burden, treatment fatigue, and reduced quality of life.
💊 Management
| Area |
Interventions |
Notes |
| Specialist care 🏥 |
Management through a specialist CF multidisciplinary team |
Core NICE principle |
| Airway clearance 🫁 |
Chest physiotherapy, airway clearance techniques, oscillating PEP, exercise, nebulised therapies where indicated |
Daily long-term treatment |
| Mucolytics 💨 |
Dornase alfa; nebulised hypertonic saline where appropriate |
Used to improve sputum clearance and reduce exacerbations |
| Antibiotics 💊 |
Oral, inhaled, or IV antibiotics guided by symptoms, microbiology, and specialist advice |
Long-term inhaled antibiotics may be used for chronic Pseudomonas |
| Macrolide therapy |
Azithromycin may be used long term in selected patients |
Can reduce exacerbation frequency and has anti-inflammatory effects |
| Nutrition 🍽️ |
Pancreatic enzyme replacement therapy (PERT), high-energy diet, fat-soluble vitamin supplements |
Essential for growth, lung health, and overall outcomes |
| CFTR modulators 🧬 |
Examples include ivacaftor, lumacaftor/ivacaftor, tezacaftor/ivacaftor, and elexacaftor/tezacaftor/ivacaftor |
Eligibility depends on genotype and commissioning arrangements |
| Complication management |
Monitor and treat CFRD, liver disease, bone disease, sinus disease, fertility issues |
Regular screening is important |
| Advanced disease |
Assessment for lung transplantation when appropriate |
Consider in progressive advanced lung disease |
| Psychosocial support ❤️ |
Mental health support, counselling, education, transition planning, social support |
Important because treatment burden is high |
📚 References
- NICE guideline NG78: Cystic fibrosis: diagnosis and management
- Cystic Fibrosis Trust UK Registry reports and standards of care
- Specialist CF centre / MDT guidance for ongoing management
