
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Cauda equina
Related Subjects: |Back pain |AP of the Cauda equina
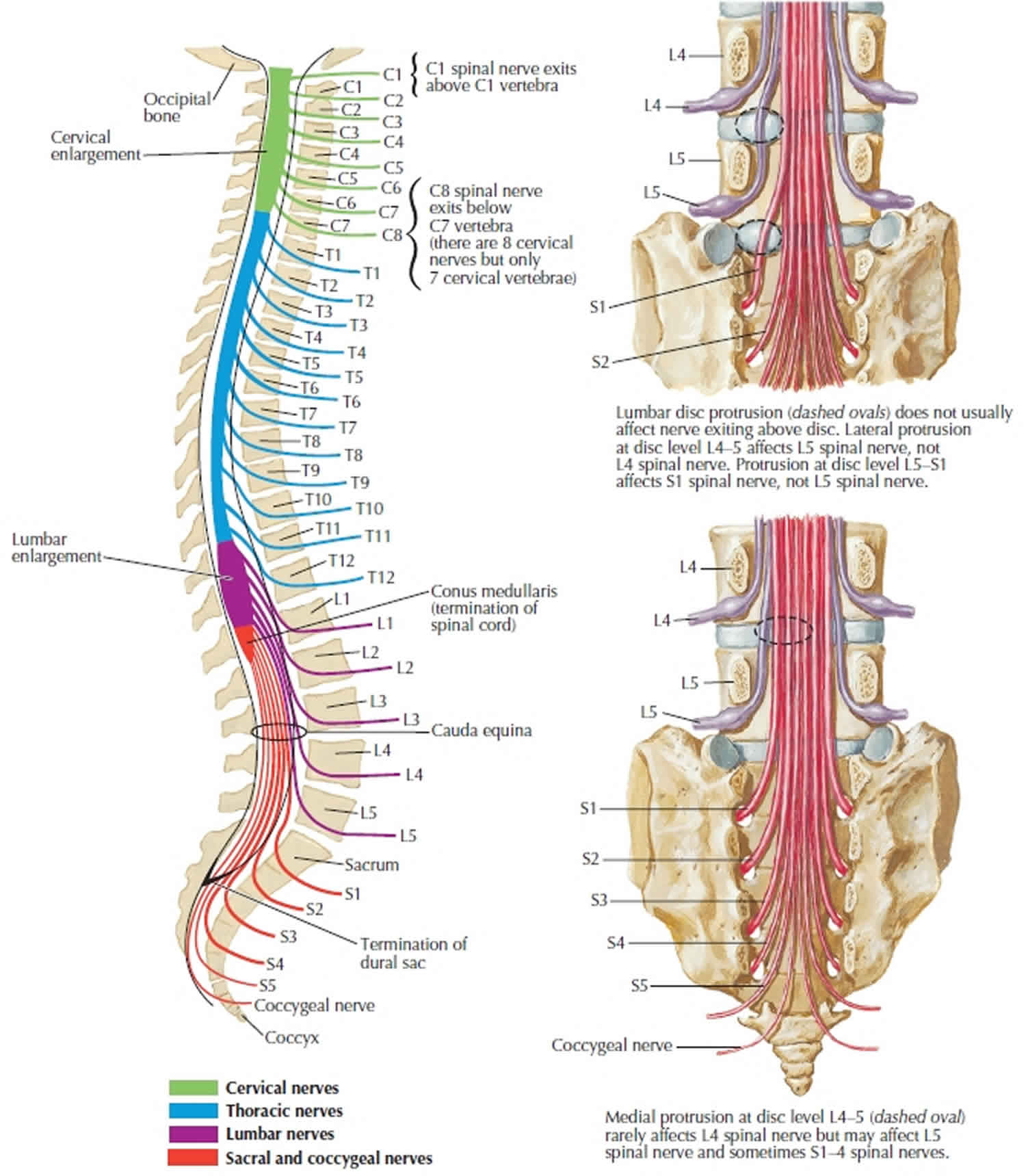
🐎 Cauda equina (“horse’s tail”) refers to the bundle of lumbar, sacral and coccygeal nerve roots that descend in cerebrospinal fluid (CSF) below the end of the spinal cord. It exists because the vertebral column grows longer than the spinal cord after early childhood, so lower roots must travel down inside the spinal canal to reach their exit foramina.
Anatomy
In adults the spinal cord typically ends as the conus medullaris around L1–L2, while the dural sac and lumbar cistern extend lower. The cauda equina sits within the lumbar cistern (CSF-filled space inside the dural sac), alongside the filum terminale (a fibrous extension that helps anchor the cord to the coccyx).
- Roots included: typically L2–L5, S1–S5, and Co1 nerve roots (ventral/motor and dorsal/sensory rootlets).
- Where they run: intradural, floating in CSF inside the thecal sac, then exit via the intervertebral foramina at their corresponding level.
- Meningeal coverings: the roots are surrounded by dura and arachnoid (forming the dural sac); CSF lies in the subarachnoid space.
- Key neighbours: posterior longitudinal ligament, intervertebral discs, facet joints, epidural venous plexus-structures that can contribute to compression when diseased.
Physiology (what the roots actually do)
- Motor (ventral roots):
- L2–L4: hip flexion/adduction, knee extension (femoral/obturator).
- L4–L5: ankle dorsiflexion and toe extension (deep peroneal).
- S1: plantarflexion, ankle reflex (Achilles), hip extension contributions.
- S2–S4: pelvic floor and external sphincters via pudendal nerve (critical for continence).
- Sensory (dorsal roots):
- Dermatomes cover lower limb sensation and the perineum; S2–S5 supply the “saddle area” (perianal/perineal/genital sensation).
- Autonomic control (the “why CES is an emergency” bit):
- Parasympathetic (S2–S4): detrusor contraction and coordinated voiding; also contributes to erection.
- Somatic (S2–S4): external urethral/anal sphincters and pelvic floor control.
- Sympathetic (T11–L2, via hypogastric plexus): bladder neck/urethral tone and ejaculation; while not in the cauda equina itself, cauda equina damage disrupts the integrated circuitry needed for continence and sexual function.
Why the cauda equina is vulnerable
Because these roots are long, mobile, and share a confined canal with discs, ligaments, and epidural veins, a relatively small increase in canal compromise can abruptly impair multiple roots at once. Compression first causes conduction block and ischaemia (reversible if relieved), but prolonged pressure triggers axonal injury and Wallerian degeneration-this is why delays can leave permanent bladder/bowel/sexual dysfunction.
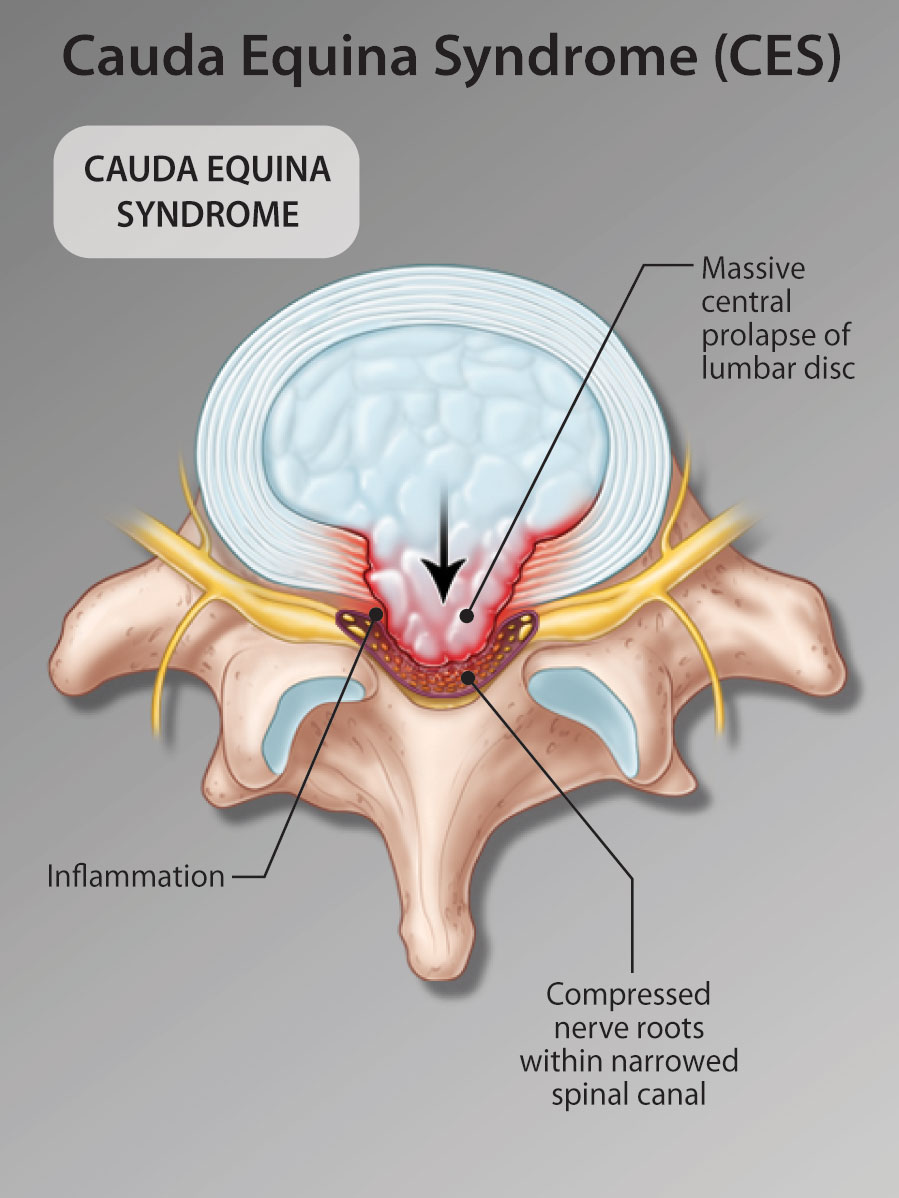
Clinical significance: Cauda Equina Syndrome (CES)
Cauda equina syndrome is a rare but high-stakes presentation of severe compression of multiple lumbosacral roots. NICE’s suspected neurological conditions guidance links to national NHS pathways for CES decision-making and escalation, emphasising urgent recognition and referral.
- Common causes:
- Large central lumbar disc prolapse (classic), spinal stenosis, tumour/metastasis, epidural abscess, haematoma, trauma, postoperative complications.
- Red-flag symptoms (act now):
- New urinary dysfunction: difficulty initiating micturition, impaired sensation of urinary flow, or painless retention ± overflow.
- Saddle sensory change: altered perianal/perineal/genital sensation (S2–S5).
- Progressive bilateral neurology: worsening bilateral radicular pain, major motor weakness (e.g., dorsiflexion), or escalating numbness.
- Bowel/sexual dysfunction: loss of rectal fullness sensation, faecal incontinence, erectile/ejaculatory dysfunction.
- UK pathway essentials (practical):
- Emergency referral to a site with emergency MRI is recommended for back/leg pain plus recent onset or deterioration of CES symptoms.
- Bladder scan can support assessment but must not be used alone to rule out CES.
- National pathway targets emergency MRI ASAP (certainly within 4 hours of request) where services provide it.
- NG59 (low back pain/sciatica) explicitly excludes CES and reminds clinicians to recognise it as an emergency requiring specialist pathways.
Summary
The cauda equina is the intradural “tail” of lumbosacral nerve roots below the conus, responsible for lower-limb motor/sensory function and-crucially-S2–S4 bladder, bowel and sexual control. Its long roots in a tight canal make it vulnerable to compressive lesions; when multiple roots are compromised, CES is a time-critical emergency because prolonged compression converts potentially reversible conduction block into permanent axonal injury. UK guidance highlights urgent escalation and emergency MRI pathways when red flags are present.
References (UK guidance & pathways)
- NICE NG127: Suspected neurological conditions: recognition and referral (last updated 2 Oct 2023).
- NICE NG127 resource: Interactive care pathway for cauda equina syndrome (links to national NHS pathways).
- GIRFT / NHS England: National Suspected Cauda Equina Pathway (Feb 2026).
- NICE NG59: Low back pain and sciatica in over 16s (notes CES/progressive deficit sit outside NG59).
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery