Lung Empyema
🫁 Pleural infection / empyema: A respiratory physician should be involved early, and thoracic surgical input should be sought if there is poor drainage, persistent sepsis, significant loculation or failure to improve. Patients requiring chest tube drainage need careful monitoring, repeat imaging and escalation planning.
ℹ️ About
- Pleural empyema is pus in the pleural cavity, often due to bacterial infection and complication of pneumonia,
- It progresses from a simple parapneumonic effusion to a complicated effusion and then frank empyema.
- The infected pleural fluid becomes acidic, glucose-depleted and loculated, making antibiotics alone insufficient.
🧬 Aetiology
- Chest sources
- Post-pneumonia parapneumonic effusion
- Aspiration pneumonia
- Penetrating chest trauma
- Oesophageal rupture
- Thoracic surgery
- Previous chest drain or pleural procedure
- Bronchopleural fistula or lung abscess rupture into the pleural space
- Abdominal sources
- Subphrenic abscess
- Pancreatitis
- Intra-abdominal sepsis tracking through the diaphragm
- Other causes
- Tuberculosis
- Haematogenous spread in severe bacteraemia
- Rarely fungal infection, especially in immunocompromised patients
⚠️ Risk Factors
- Older age, frailty or poor physiological reserve
- Stroke, dementia, reduced consciousness or dysphagia
- Aspiration risk, alcohol excess, reflux or poorly controlled epilepsy
- Diabetes mellitus
- Immunosuppression, malignancy or chemotherapy
- Intravenous drug use
- Poor dentition or periodontal disease
- Recent pneumonia, thoracic surgery, trauma or pleural procedure
🔍 Clinical Features
- Recent or partially treated pneumonia with persistent fever or inflammatory response
- Fever, rigors, malaise, anorexia, weight loss or night sweats
- Pleuritic chest pain
- Dyspnoea or increasing oxygen requirement
- Cough, sometimes with purulent or foul-smelling sputum
- Reduced chest expansion, dull percussion note and reduced breath sounds over an effusion
- Features of sepsis: tachycardia, hypotension, delirium, AKI or raised lactate
🧫 Common Organisms
- Community-acquired pleural infection
- Streptococcus pneumoniae
- Streptococcus anginosus group, including S. intermedius and S. constellatus
- Staphylococcus aureus
- Anaerobes, especially with aspiration or poor dentition
- Enterobacteriaceae such as Escherichia coli, particularly in frailty or comorbidity
- Hospital-acquired pleural infection
- Staphylococcus aureus, including MRSA depending on local risk
- Gram-negative organisms such as E. coli, Klebsiella and Pseudomonas aeruginosa
- Anaerobes and mixed infection
- TB empyema should be considered with chronic symptoms, exposure risk, immunosuppression or compatible imaging.
- Fungal empyema is rare but important in immunocompromised patients or after oesophageal/gastrointestinal contamination.
🔎 Differential Diagnosis
- Simple parapneumonic effusion — sterile fluid associated with pneumonia; may resolve with antibiotics alone.
- Complicated parapneumonic effusion — infected or biochemically hostile fluid; often needs drainage.
- Lung abscess — cavitating infection within lung parenchyma rather than pleural space.
- Pulmonary embolism — pleuritic pain, hypoxia and small effusion can mimic infection.
- Malignancy — especially unilateral, recurrent or non-resolving effusion/consolidation.
- Tuberculosis — chronic systemic symptoms, lymphocytic effusion or epidemiological risk.
- Heart failure — usually bilateral transudative effusions but may coexist with pneumonia.
🧪 Investigations
- Blood tests: FBC, U&E, LFT, CRP, clotting, glucose and venous/arterial blood gas if unwell.
- Microbiology: blood cultures before antibiotics; sputum culture if productive; consider viral testing.
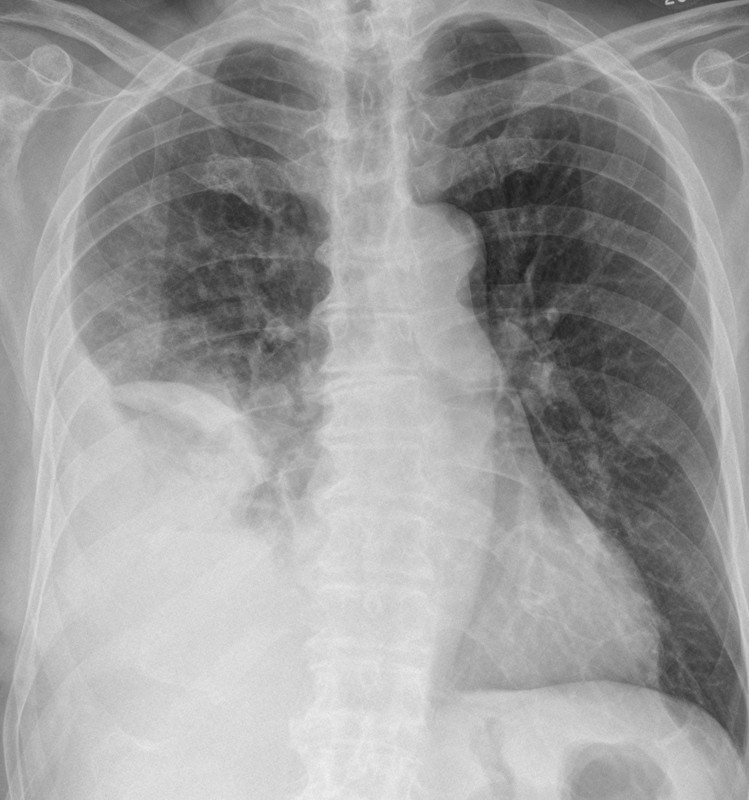
- Chest X-ray: may show consolidation, pleural effusion, pleural opacity or loculation.
- Thoracic ultrasound: confirms pleural fluid, assesses septations/loculations and guides safe aspiration or drain placement.
- Diagnostic pleural aspiration: send for pH, glucose, LDH, protein, Gram stain, culture, cytology if indicated, and AFB/TB culture if suspected.
- CT chest with contrast: useful if diagnosis is uncertain, drainage is poor, loculation is suspected, malignancy is possible, or surgery is being considered.
🧪 Pleural Fluid Clues
- Frank pus confirms empyema and requires drainage.
- Positive Gram stain or culture supports pleural infection and usually requires drainage.
- Low pH suggests complicated parapneumonic effusion and need for chest drainage.
- Low glucose and high LDH support complicated infection.
- Loculated pleural fluid suggests poor spontaneous drainage and higher risk of treatment failure.
💊 Management
- Initial assessment: ABCDE, oxygen if hypoxic, sepsis assessment, analgesia, IV access and early senior review.
- Antibiotics: start prompt empirical therapy after cultures where possible, covering typical organisms and anaerobes; follow local guidelines and microbiology advice.
- Drain infected fluid: chest tube drainage is needed for frank pus, positive microbiology, low pleural pH, significant loculation or poor clinical progress. Small-bore drains are now widely accepted for initial drainage, and persistent residual collection may need combined intrapleural tPA/DNase or surgical escalation. As regards chest drain size: small-bore image-guided drains are commonly used; flush regularly according to local protocol to reduce blockage risk.
- Analgesia and sedation: provide adequate local anaesthetic and analgesia; consider anxiolysis/opioid premedication where appropriate and safe.
- Review response: monitor fever, oxygen requirement, pain, drain output, CRP/WCC, renal function and repeat imaging.
- Intrapleural therapy: consider combined intrapleural tPA and DNase if drainage is inadequate and there is residual infected collection, with respiratory specialist input.
- Surgical referral: discuss with thoracic surgery if persistent sepsis, trapped lung, organised empyema, bronchopleural fistula or failure of medical drainage.
- Supportive care: VTE prophylaxis, nutrition, hydration, diabetes control, physiotherapy and management of aspiration risk.
- TB possibility: if TB is suspected, send appropriate samples and involve respiratory/TB specialists before committing to a treatment pathway.
⚠️ Complications
- Sepsis and multi-organ dysfunction
- Respiratory failure
- Loculated pleural infection and trapped lung
- Bronchopleural fistula and pyopneumothorax
- Empyema necessitans: extension through the chest wall causing subcutaneous abscess or fistula
- Purulent pericarditis
- Extension through the diaphragm causing peritonitis or subphrenic infection
- Metastatic infection such as meningitis, septic arthritis or osteomyelitis
- Chronic pleural thickening and reduced lung function
💊 Empirical Antibiotics for Pleural Infection / Empyema
- Always check local antimicrobial guidelines and renal function.
- Take blood cultures and pleural fluid samples before antibiotics if this does not delay treatment.
- Seek microbiology advice if severe sepsis, hospital-acquired infection, MRSA risk, immunosuppression, TB risk, renal failure or penicillin allergy.
🏠 Community-Acquired Pleural Infection
- Typical first-line: Co-amoxiclav 1.2 g IV every 8 hours.
- If very severe / septic: discuss with microbiology; broader Gram-negative cover may be needed.
- Step-down when improving: Co-amoxiclav 625 mg PO every 8 hours, if cultures and clinical picture are suitable.
🏥 Hospital-Acquired Pleural Infection
- Typical first-line if severe or late hospital-acquired: Piperacillin-tazobactam 4.5 g IV every 8 hours.
- If MRSA risk: add vancomycin or teicoplanin as per local policy and drug-level monitoring.
- If ESBL risk or recent broad-spectrum antibiotics: discuss urgently with microbiology; meropenem may be needed.
⚠️ Penicillin Allergy
- Minor non-severe rash history: Cefuroxime 1.5 g IV every 8 hours plus metronidazole 500 mg IV/PO every 8 hours may be used in some local guidelines.
- Severe immediate allergy / anaphylaxis: discuss with microbiology; options may include levofloxacin plus metronidazole, or vancomycin-based combinations depending on risk profile.
⏱️ Duration
- Usually a prolonged course, commonly around 2–6 weeks total, guided by clinical response, CRP, imaging, drainage success and microbiology advice.
- Switch IV to oral once the patient is clinically improving, afebrile or settling, able to absorb orally, and source control is adequate.
🚩 Escalation / Specialist Input
- Respiratory physician for all suspected pleural infection requiring drainage
- Microbiology for antibiotic choice, resistant organisms, TB concern or failure to improve
- Thoracic surgery for persistent sepsis, poor drainage, organised empyema or suspected bronchopleural fistula
- ITU if severe hypoxia, septic shock, rising lactate, respiratory fatigue or multi-organ dysfunction
📚 References