Malignant MCA syndrome ✅
Related Subjects:
|Acute Stroke Assessment (ROSIER&NIHSS)
|Causes of Stroke
|Ischaemic Stroke
|Cancer and Stroke
|Cardioembolic stroke
|CT Basics for Stroke
|Acute Hydrocephalus
🧠 Introduction
- ⚡ Malignant MCA syndrome occurs after a large MCA territory infarct, leading to massive cerebral oedema and risk of herniation.
- 🕐 Typically presents 2–5 days post-stroke, but severe oedema can develop within 24h.
- 🔍 Pathophysiology: cytotoxic oedema → midline shift → raised ICP → risk of transtentorial herniation.
- 📊 Clinical trials demonstrate that early decompressive surgery reduces mortality; survivors often have significant disability (mRS 4–5).
🧬 Aetiology
- 🫀 Large vessel atheroembolism (MCA stem or ICA terminus).
- 💓 Cardioembolism (atrial fibrillation, valvular disease, LV thrombus).
- 🩸 Carotid or MCA dissection → embolism to MCA territory.
🩺 Clinical Presentation
- Contralateral hemiparesis, hemianopia, hemisensory loss ± aphasia/neglect (depends on dominant hemisphere involvement).
- Progressive decline in consciousness due to mass effect and raised ICP.
- Late signs: ipsilateral pupillary dilatation, Cheyne-Stokes respiration, signs of uncal or transtentorial herniation.
🖼️ Imaging
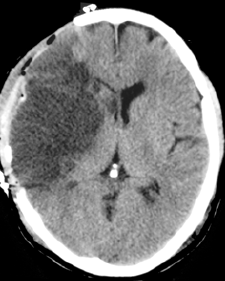

- CT Head: May be normal early; later shows hypodensity >50% MCA territory, mass effect, midline shift, sulcal effacement.
- MRI DWI: Accurate infarct volume measurement; >145 cm³ predicts poor outcome without intervention.
- CTA: Assess vessel patency, rule out tandem ICA/MCA occlusion.
📑 RCP / NICE Guidance
Consider decompressive hemicraniectomy in adults with malignant MCA infarction if:
- Pre-stroke mRS <2 (functionally independent).
- Clinical MCA syndrome with NIHSS >15.
- Reduced consciousness (NIHSS 1a ≥1).
- Imaging: infarct >50% MCA territory or DWI volume >145 cm³.
- Age <60 yrs generally; selected patients >60 yrs may benefit (DESTINY II).
💊 Management
- 🎯 Supportive ICP measures: intubation, sedation, osmotherapy (mannitol, hypertonic saline), controlled hyperventilation – not sufficient alone.
- 🔪 Decompressive hemicraniectomy + durotomy: Large bone flap & dural opening; allows brain expansion, prevents herniation, reduces mortality.
- 👥 Patient selection: consider age, comorbidities, baseline function, patient/family wishes.
- ⚠️ Poor prognostic features: infarct extends to ACA/PCA territories, very large infarct volume, refractory ICP.
- 📊 Evidence from trials:
- HAMLET – surgery <48h ↓ mortality; delayed >96h less effective.
- DESTINY I – younger patients had marked survival benefit.
- DESTINY II – ≥60 yrs, survival benefit, but most survivors dependent (mRS 4–5).
- 🧪 Medical adjuncts: maintain normothermia, normoglycaemia, normovolaemia; seizure prophylaxis if indicated; close ICU monitoring.
📝 Exam / Student Tips
- ⚡ Recognise early malignant MCA features: massive hemiplegia, dysphasia/neglect, declining consciousness, severe headache/ICP symptoms.
- 🧠 CT hypodensity >50% MCA territory or DWI volume >145 cm³ = classic red flag for neurosurgical referral.
- 📆 Timing is critical: surgery <48h gives best survival.
- 💭 Know trial names & outcomes (HAMLET, DESTINY I/II) – common OSCE/finals knowledge point.
- 👨⚕️ Always combine imaging findings with clinical status; early discussion with neurosurgery is key.
📚 References / Evidence
| 🧪 Trial |
👨⚕️ Authors |
📊 Key Outcome |
| HAMLET (Lancet Neurol. 2009) |
HAMLET investigators |
Hemicraniectomy within 48h ↓ mortality; late surgery (>96h) offers minimal benefit. |
| DESTINY I (Stroke 2007) |
DESTINY Study Group |
Surgery markedly ↓ mortality in younger adults; trial stopped early after meta-analysis with DECIMAL & HAMLET. |
| DESTINY II (NEJM 2014) |
DESTINY II Investigators |
Adults ≥60 yrs: surgery ↑ survival but most survivors had severe disability (mRS 4–5). |
