
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Wolff-Parkinson White syndrome (WPW) AVRT ✅
Related Subjects: |Electrical Storm (Recurrent VT/VF) |Wolff-Parkinson White syndrome (WPW) AVRT |Lown Ganong Levine Syndrome AVRT |Supraventricular Tachycardia (SVT) |Atrioventricular Nodal Reentrant Tachycardia AVNRT |Atrial Flutter |Atrial Fibrillation |Sinus Tachycardia |Sinus Arrhythmia |Multifocal Atrial Tachycardia |Resuscitation - Adult Tachycardia Algorithm
⚡ Wolff-Parkinson-White (WPW) Syndrome is caused by an accessory conduction pathway (Bundle of Kent) bypassing the AV node. This can trigger reentrant tachycardias (AVRT) and, if atrial fibrillation conducts rapidly down the accessory pathway, life-threatening ventricular fibrillation 🚨.
| Arrhythmia | Acute Management (Guideline-Compliant) |
|---|---|
| Stable Orthodromic AVRT
(narrow-complex regular SVT) |
|
| Unstable AVRT (shock, syncope, hypotension, ischaemia) |
|
| Pre-excited AF – unstable
(irregular wide-complex, HR often >220 bpm) |
|
| Pre-excited AF – stable |
|
| Absolutely contraindicated in pre-excited AF |
|
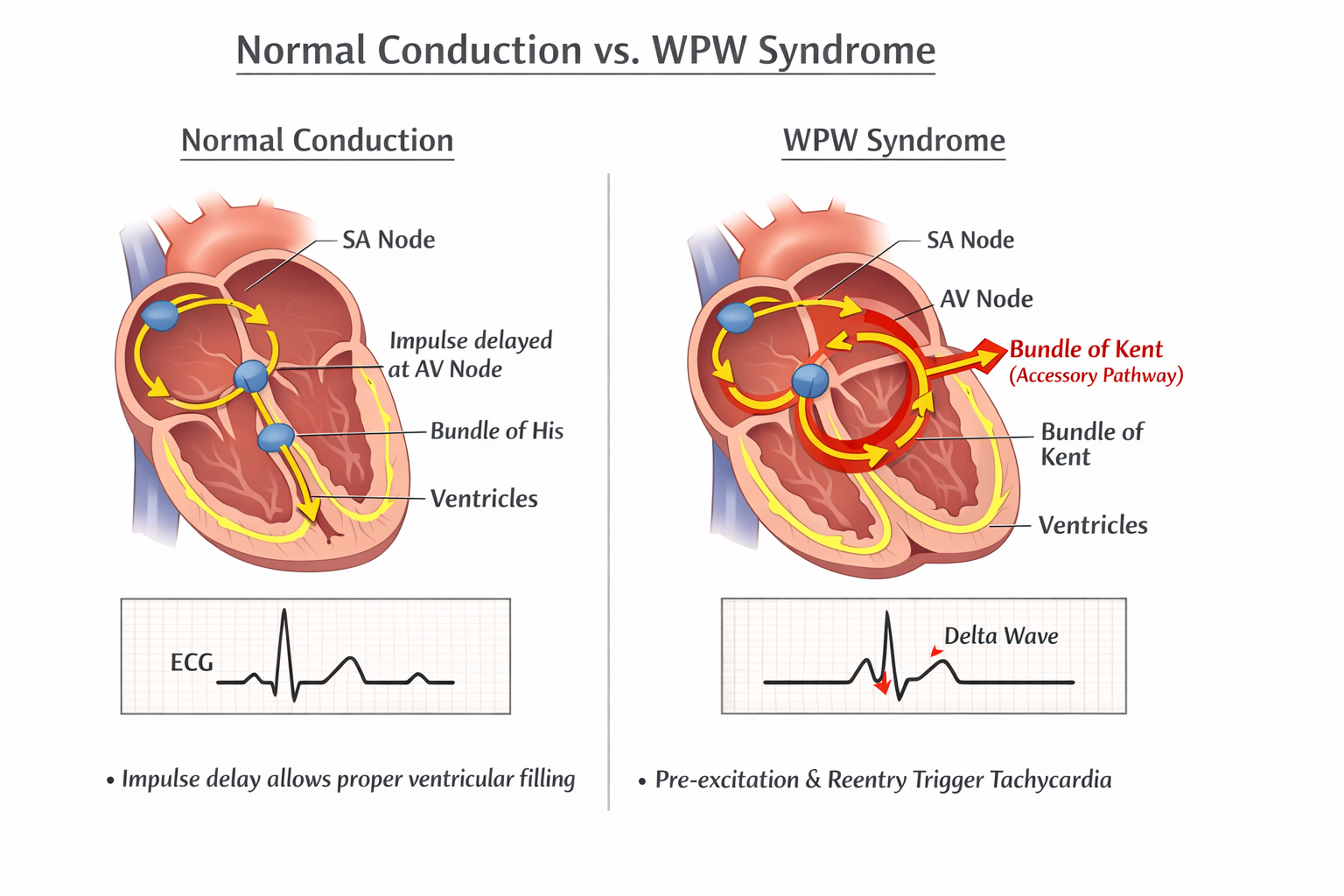
🧠 Pathophysiology & Mechanisms
- 💓 Accessory pathway: Bundle of Kent provides direct atrioventricular conduction, bypassing the AV node delay.
- ⏱ Normally, the AV node slows conduction to allow ventricular filling; in WPW, impulses may conduct rapidly, causing early ventricular depolarisation (delta wave).
- 🔄 Reentry circuits: Impulses can travel down the AV node and return via the accessory pathway, triggering AVRT (orthodromic or antidromic).
- ⚡ Pre-excited AF: Rapid atrial impulses conducted through the accessory pathway can precipitate ventricular fibrillation (VF) – life-threatening emergency.
- 🧬 Genetic predisposition: Mutations affecting cardiac conduction tissue have been described; familial WPW reported, especially with HCM or Ebstein anomaly.
🫀 Causes / Predisposing Conditions
- 🧒 Congenital structural abnormalities:
- ASD (secundum type)
- Ebstein anomaly (apical displacement of tricuspid valve)
- Ventricular pre-excitation in hypertrophic cardiomyopathy (HCM)
- 🧬 Genetic syndromes:
- Familial WPW (rare)
- PRKAG2 mutation – glycogen storage cardiomyopathy with pre-excitation
- 🦠 Acquired / structural heart changes (rare):
- Myocarditis causing transient conduction abnormalities
- Post-surgical accessory pathways after congenital repair
- Idiopathic – most WPW patients have no identifiable structural heart disease.
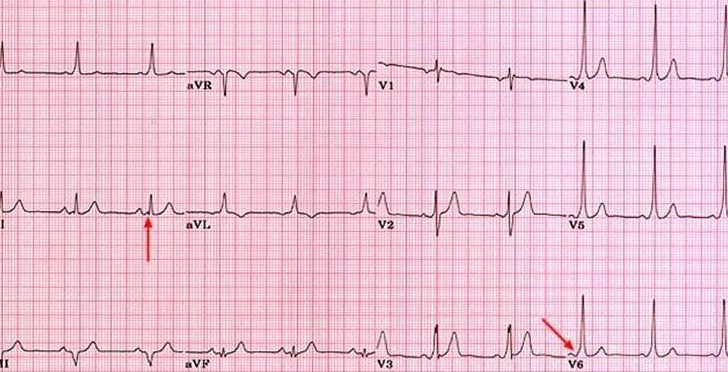
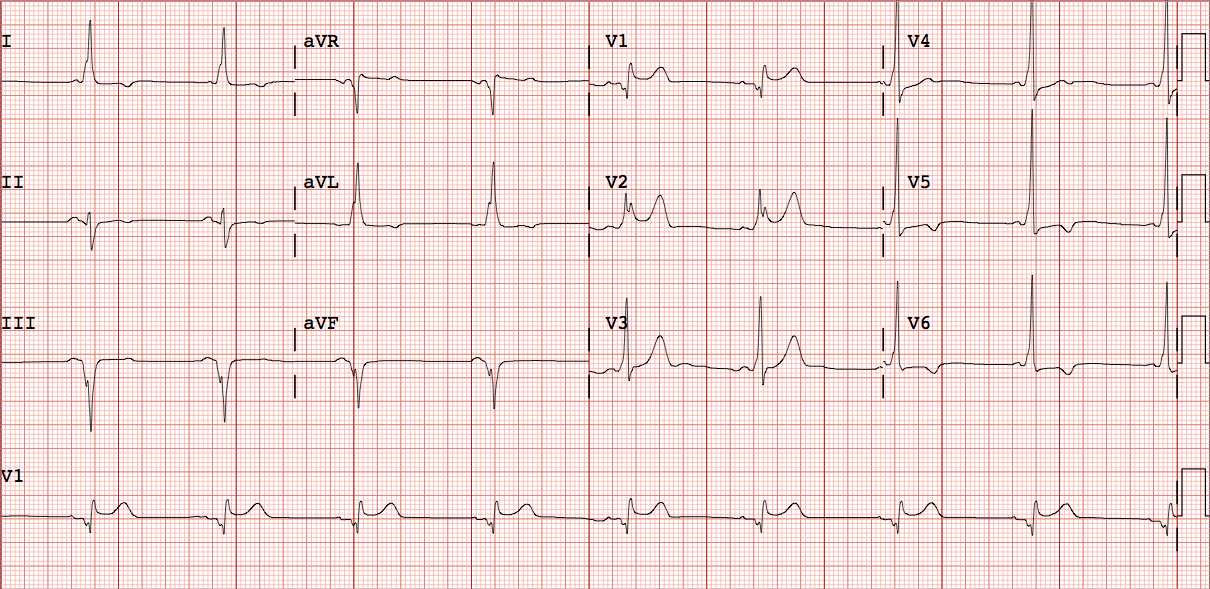
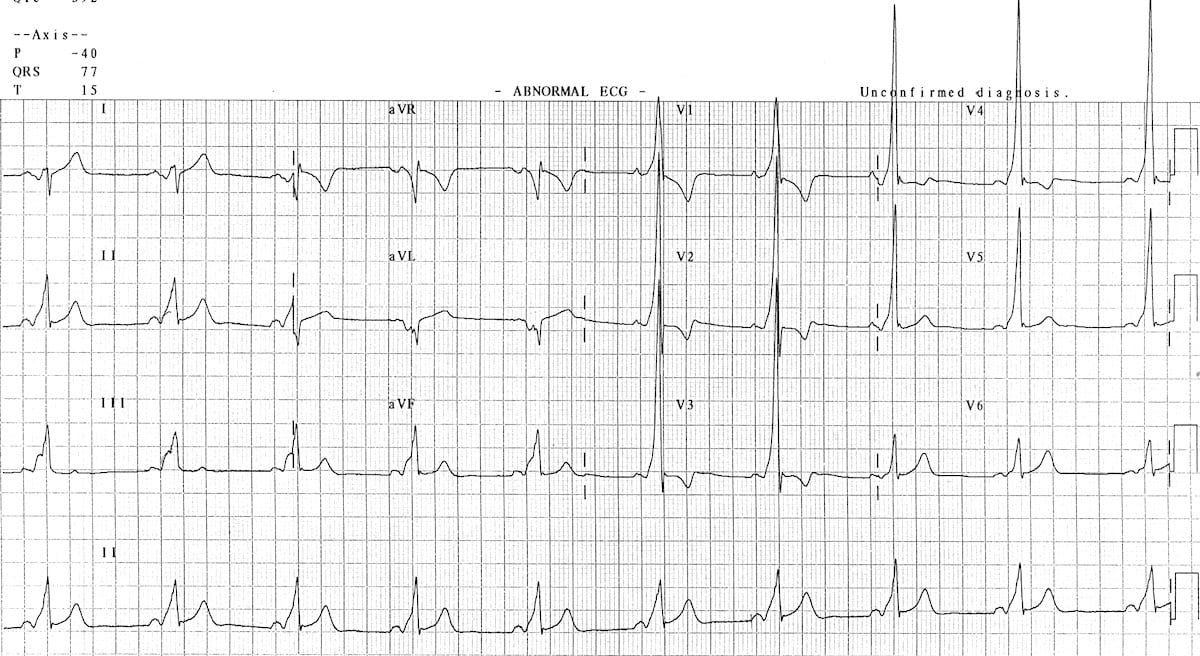
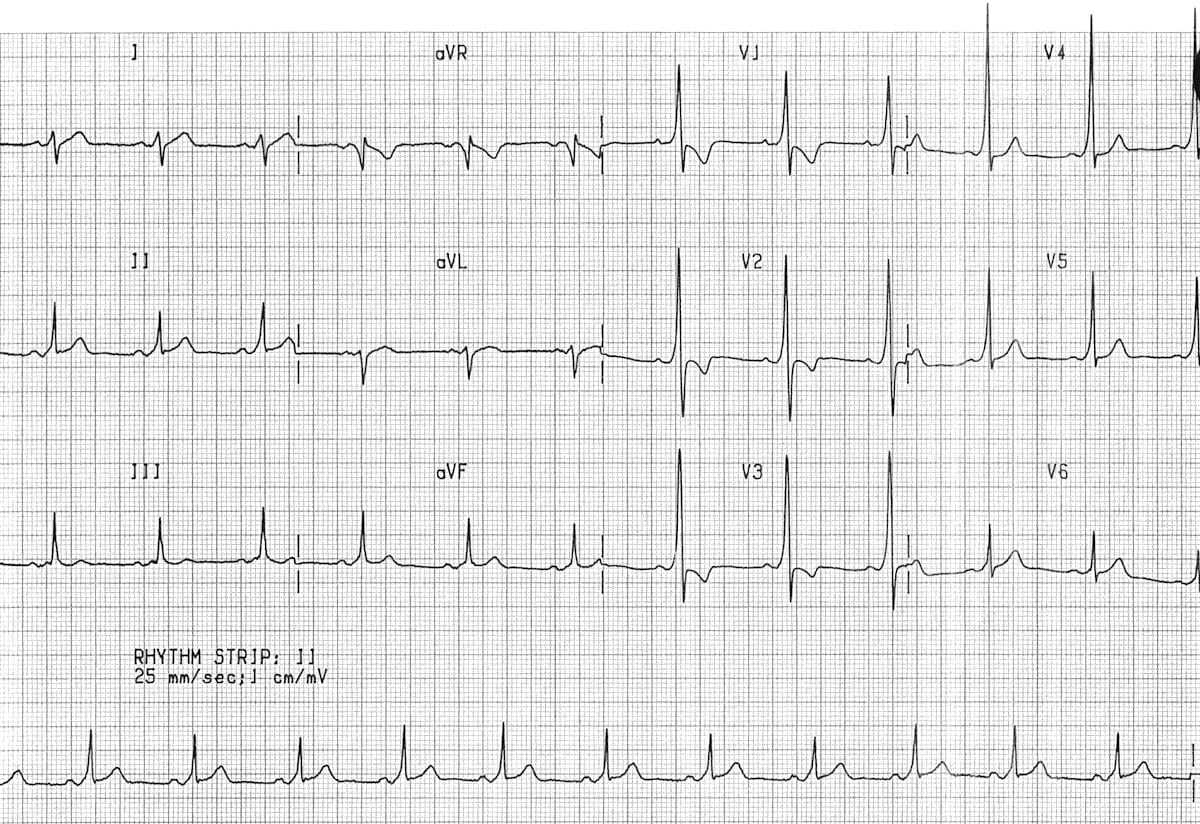
📈 ECG Features
- Manifest pathway: Short PR + delta wave
- Concealed pathway: Normal ECG, no delta wave
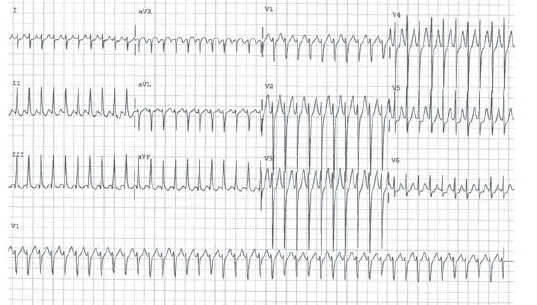
- Arrhythmias: AVRT (narrow complex), AF with pre-excitation (irregular wide complex)
🔎 Investigations
- 🧪 Bloods: FBC, U&E, TFTs, CRP
- 📈 ECG: delta wave, short PR, pre-excitation
- 🫀 Echo / MRI: structural heart disease
- ⚡ EP study: localise accessory pathway, plan ablation
💀 Mortality in Wolff-Parkinson-White (WPW) Syndrome: Overall, WPW carries a low annual mortality (~0.1% per year) in asymptomatic patients. The main risk is sudden cardiac death (SCD) from rapid conduction of atrial fibrillation down the accessory pathway, potentially causing ventricular fibrillation. Risk is higher in patients with a short accessory pathway refractory period (<250 ms), a history of syncope or cardiac arrest, multiple accessory pathways, or younger age (<30 years) with AF episodes. Symptomatic individuals or those with high-risk features should be considered for electrophysiology evaluation and catheter ablation.
📊 WPW Mortality Risk Factors
| Risk Factor | Impact on Mortality / SCD Risk |
|---|---|
| History of syncope | ↑ Risk of sudden cardiac death (SCD) |
| Previous cardiac arrest or ventricular fibrillation | Highest risk – urgent ablation recommended |
| Short accessory pathway refractory period (<250 ms) | ↑ Rapid conduction during AF → VF risk |
| Multiple accessory pathways | ↑ Arrhythmia recurrence & SCD risk |
| Young age (<30 years) with documented AF | Moderate ↑ risk of SCD |
| Asymptomatic with long refractory pathway | Low annual mortality (~0.1% per year) |
💡 Note: Symptomatic patients or those with high-risk features should be referred for electrophysiology study and catheter ablation. 📚 References: Pappone C, et al. Circulation 2003;108:2286–2291; Chen SA, et al. J Cardiovasc Electrophysiol 2001;12:1282–1291; ESC Guidelines, Eur Heart J 2019;40:1573–1601.
🏥 Definitive Management of WPW Syndrome
- 🎯 Radio-frequency catheter ablation (RFCA)
- First-line treatment for patients with recurrent symptomatic SVT or high-risk accessory pathways (short refractory period, prior syncope, or documented pre-excited AF).
- Success rates are high: ~95–98% for single accessory pathway ablation.
- Reduces risk of sudden cardiac death by eliminating pre-excitation and preventing rapid conduction during AF.
- Procedure involves mapping the accessory pathway and delivering RF energy to interrupt conduction.
- ⚠️ Complications are rare but may include:
- AV block (~1%) → may require permanent pacemaker
- Vascular injury at access site (femoral vein/artery)
- Pericardial effusion or tamponade (<1%)
- Arrhythmia recurrence (~3–5%) requiring repeat ablation
- Pre-procedural considerations: anticoagulation if AF present, review antiarrhythmic drugs, baseline ECG and echocardiography.
- Post-procedure: monitor for arrhythmia recurrence, ECG follow-up, advise patients regarding symptom recognition.
- 💊 Medical Therapy (Adjunct / Bridging)
- For patients awaiting ablation, or those not suitable for procedure. Options include:
- Class Ic antiarrhythmics (Flecainide, Propafenone) for AVRT prevention in structurally normal hearts
- Amiodarone if other antiarrhythmics contraindicated or in patients with structural heart disease
- Not first-line due to lower efficacy and potential long-term toxicity.
- For patients awaiting ablation, or those not suitable for procedure. Options include:
- 🩺 Indications for Catheter Ablation
- Symptomatic WPW with recurrent SVT.
- High-risk features: prior syncope, short refractory pathway, history of pre-excited AF.
- Occupational risk: pilots, athletes, military personnel.
- Asymptomatic patients may be considered if EPS demonstrates high-risk pathway characteristics.
- 🧾 Alternative / Surgical Approaches
- Rarely, surgical ablation is used if RF ablation fails or anatomy is unsuitable.
- Maze procedure during concomitant cardiac surgery may incidentally eliminate accessory pathways.
- 📋 Follow-up
- Post-ablation ECG to confirm loss of pre-excitation.
- Holter monitoring in selected patients to detect recurrent arrhythmias.
- Long-term prognosis excellent: low recurrence and normalized risk of SCD.
- Patient education: recognize palpitations, syncope, or irregular pulse as triggers for prompt evaluation.
🩺 Case Examples
Case 1 – Stable SVT in WPW: 24yo man, palpitations, HR 180 bpm, ECG shows narrow-complex tachycardia, previous delta wave. Management: 💊 Procainamide or flecainide; consider ablation. ❌ Avoid AV nodal blockers (adenosine/verapamil/beta-blockers/digoxin in pre-excited AF).
Case 2 – Pre-excited AF: 32yo woman, HR >200 bpm, irregular wide QRS, stable. Management: 💊 IV Procainamide or Ibutilide; DC cardioversion if unstable; EP referral for ablation. ❌ Avoid AV nodal blockers.
Case 3 – Incidental WPW: 19yo asymptomatic, ECG shows delta wave. Management: 🩺 No acute treatment; counsel; risk stratify with EP study; ablation if high-risk occupation. ❌ Avoid ignoring risk in athletes/pilots.
⚠️ Safety Tip: Always distinguish **pre-excited AF from regular SVT** – AV nodal blockers in pre-excited AF can trigger ventricular fibrillation.
📚 References
- Brugada J, et al. ESC Guidelines for the management of supraventricular tachycardia. Eur Heart J. 2019;40:1573–1601.
- Pappone C, et al. Radiofrequency catheter ablation in WPW syndrome: long-term follow-up. Circulation. 2003;108:2286–2291.
- Chen SA, et al. Electrophysiologic characteristics and management of WPW. J Cardiovasc Electrophysiol. 2001;12:1282–1291.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery