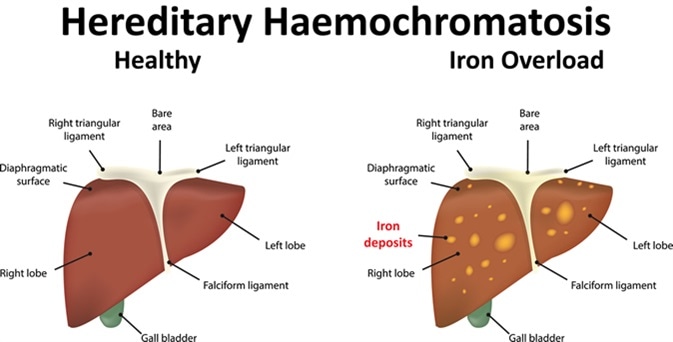
Hereditary Haemochromatosis
Related Subjects:
| Chronic liver disease
| Cirrhosis
| Alkaline phosphatase (ALP)
| Liver Function Tests
| Ascites Assessment and Management
| Budd-Chiari syndrome
| Autoimmune Hepatitis
| Primary Biliary Cirrhosis
| Primary Sclerosing Cholangitis
| Wilson disease
| Hereditary Haemochromatosis
| Alpha-1 Antitrypsin (AAT) deficiency
| Nonalcoholic steatohepatitis (NASH)
| Spontaneous Bacterial Peritonitis
| Alcoholism and Alcoholic Liver Disease
|Hepatitis C
💡 Hereditary haemochromatosis (HH) is the most common inherited cause of iron overload.
Early recognition and venesection treatment can prevent cirrhosis, diabetes, and cardiomyopathy.
📘 About
- Autosomal recessive disorder of excessive intestinal iron absorption → progressive iron overload.
- No regulated excretion mechanism → iron accumulates in liver, pancreas, heart, joints, skin.
- Most common cause of primary liver disease in Western populations.
- Classic triad: “Bronze diabetes” = cirrhosis + diabetes + skin pigmentation.
🧬 Genetics
- HFE gene mutation (chromosome 6).
- C282Y homozygous → high risk; C282Y/H63D compound heterozygotes milder.
- Carrier frequency: ~1 in 8 in Northern Europeans; homozygous prevalence 1 in 200.
- Incomplete penetrance: not all homozygotes develop disease.
⚠️ Aetiology & Pathology
- HFE mutation → loss of hepcidin regulation → unopposed ferroportin activity → ↑ iron absorption.
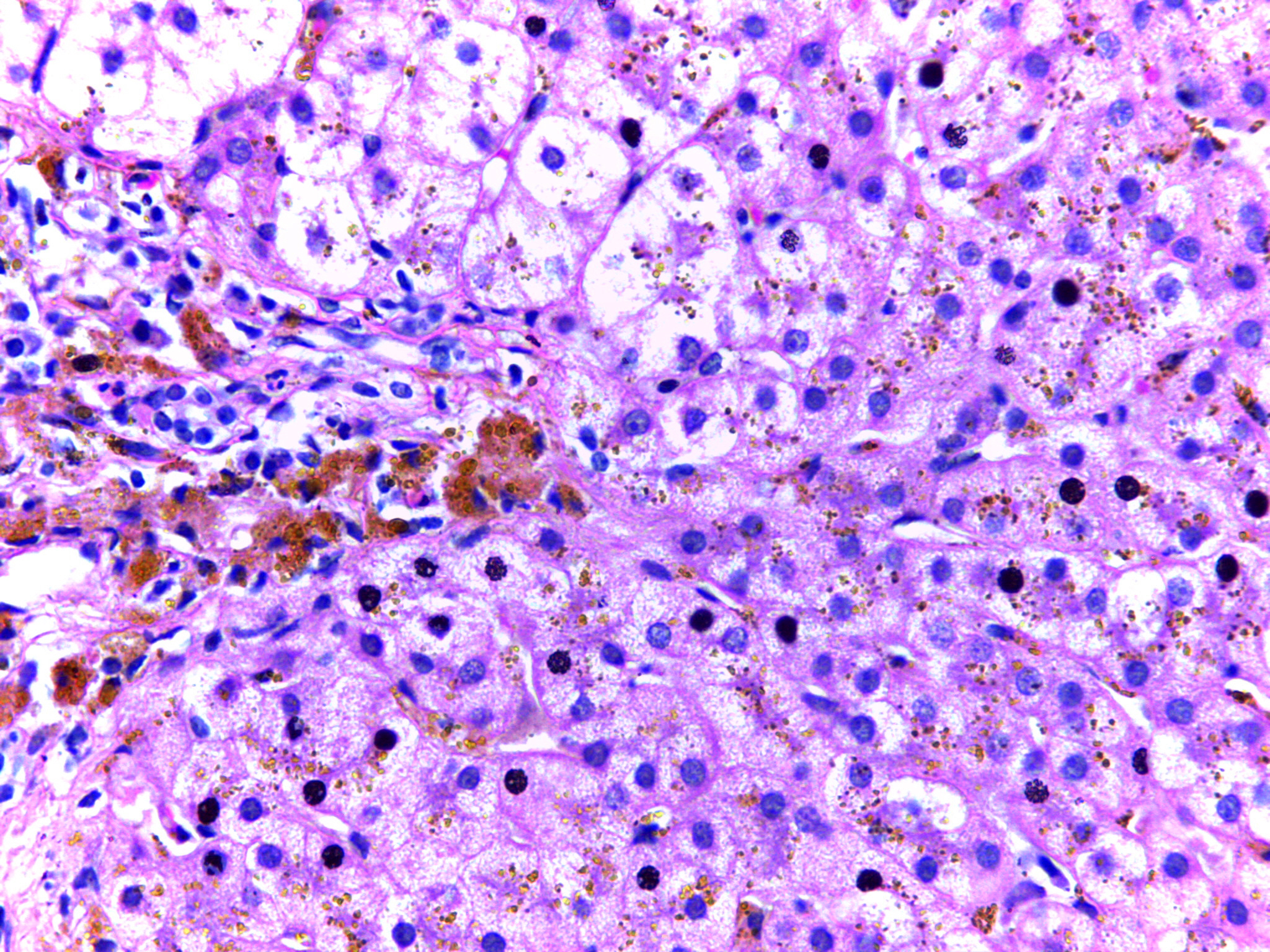
- Progressive iron deposition → hepatocyte injury, fibrosis, cirrhosis.
- Prussian Blue stain: periportal iron deposition in hepatocytes, sparing Kupffer cells.
🩺 Clinical Features
- Non-specific: fatigue, arthralgia, abdominal pain.
- Liver: hepatomegaly, cirrhosis, ↑ HCC risk.
- Pancreas: diabetes mellitus.
- Endocrine: hypogonadism, impotence, infertility.
- Cardiac: dilated/restrictive cardiomyopathy, arrhythmias, heart failure.
- Skin: slate-grey/bronze pigmentation.
- Joints: arthropathy, chondrocalcinosis (especially 2nd/3rd MCP joints).
🔎 Investigations
- Serum ferritin usually elevated (>500 µg/L).
- Transferrin saturation >50% (often >90%).
- Genetic testing for HFE mutations (C282Y, H63D).
- Liver enzymes (↑ ALT, AST), assess fibrosis with elastography.
- MRI T2*: quantifies iron in liver, pancreas, myocardium.
- Liver biopsy now rare - for unclear cases or staging cirrhosis.
📊 Summary Table
| Feature | Typical Findings |
|---|
| Genetics | C282Y homozygous or C282Y/H63D compound heterozygous |
| Biochemistry | Ferritin >500, Transferrin saturation >50% |
| Liver | Hepatomegaly, cirrhosis, ↑ HCC risk |
| Endocrine | Diabetes, hypogonadism |
| Cardiac | Cardiomyopathy, arrhythmias |
| Skin | Slate-grey / bronze pigmentation |
| Joints | Arthropathy, chondrocalcinosis |
🚨 Complications
- Cirrhosis & hepatocellular carcinoma (HCC).
- Heart failure, arrhythmias.
- Secondary diabetes.
- Hypogonadism and infertility.
👨👩👧 Screening
- Screen patients with unexplained high ferritin + transferrin saturation.
- First-degree relatives of affected patients should undergo HFE genetic testing.
- Especially relevant in Northern European ancestry.
⚕️ Management
- Venesection (phlebotomy): weekly until ferritin 20–50 µg/L, transferrin saturation <50%, then lifelong maintenance every 1–3 months.
- Iron chelation (deferoxamine, deferasirox) only if phlebotomy contraindicated (e.g. severe anaemia, cardiac failure).
- Cirrhosis: HCC surveillance (US + AFP every 6 months).
- Advise avoidance of excess alcohol, iron, and vitamin C supplementation.
📚 References
Cases - Hereditary Haemochromatosis (HH)
- Case 1 - Classic triad 🏥: A 52-year-old man presents with fatigue, arthralgia, and bronze skin pigmentation. Bloods: ferritin 1800 µg/L, transferrin saturation 75%. LFTs: raised ALT/AST. Genetic testing: homozygous C282Y mutation. Diagnosis: hereditary haemochromatosis with early organ involvement. Managed with regular venesection.
- Case 2 - Diabetes and liver disease 🍬🫁: A 60-year-old man with type 2 diabetes develops hepatomegaly and features of cirrhosis. Bloods: ferritin 2400 µg/L, iron studies show high transferrin saturation. Fibroscan: advanced fibrosis. Diagnosis: HH with “bronze diabetes” and cirrhosis. Managed with venesection, strict alcohol avoidance, and hepatology follow-up for HCC surveillance.
- Case 3 - Cardiac involvement ❤️: A 48-year-old woman presents with palpitations, exertional dyspnoea, and ankle swelling. ECG: atrial fibrillation. Echocardiogram: dilated cardiomyopathy. Iron studies: ferritin 1600 µg/L, transferrin saturation 80%. Genetic test: HFE mutation. Diagnosis: HH with iron overload cardiomyopathy. Managed with venesection, cardiology input, and rhythm control.
Teaching Point 🩺: Hereditary haemochromatosis is an autosomal recessive iron overload disorder (most often HFE C282Y mutation). It causes progressive organ damage: liver (cirrhosis, HCC), pancreas (diabetes), skin (bronzing), joints (arthropathy), and heart (cardiomyopathy, arrhythmias). Diagnosis: ↑ ferritin, ↑ transferrin saturation, genetic testing. First-line treatment: regular venesection.
