🫀 First-degree atrioventricular (AV) block is defined by a prolonged PR interval >200 ms with 1:1 AV conduction, meaning every P wave is followed by a QRS complex. It reflects delayed conduction from atria to ventricles, usually at the AV node, rather than a missed beat. In many people it is a benign ECG finding, especially in younger individuals, athletes, or during high vagal tone, but it can also occur with drugs, ischaemia, myocarditis, infiltrative disease, or electrolyte disturbance.
📖 About
- The PR interval is measured from the start of the P wave to the start of the QRS complex.
- Normal PR interval is 120-200 ms (3-5 small squares on standard ECG paper).
- First-degree AV block means the PR interval is >200 ms, but every atrial impulse is still conducted.
- It is often asymptomatic and found incidentally on ECG.
- The conduction delay is usually within the AV node, although it may occasionally be in the atria, His bundle, or conduction system.
🧠 Why it happens
- Electrical impulses travel from the SA node through the atria to the AV node, where there is normally a short physiological delay.
- In first-degree AV block, this delay is longer than normal, so ventricular activation occurs later.
- Because all impulses still get through, there are no dropped beats, unlike Mobitz I, Mobitz II, or complete heart block.
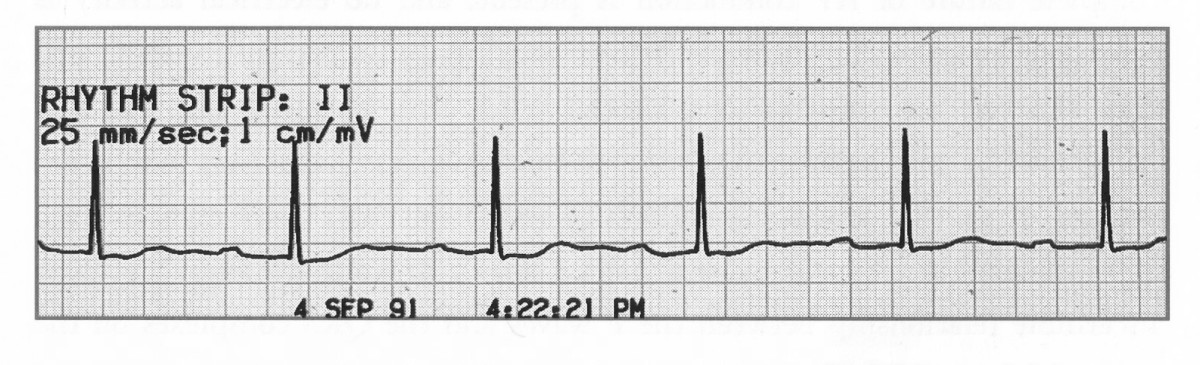
📉 ECG Features
- PR interval >0.20 seconds (>200 ms; more than 5 small squares).
- Each P wave is followed by a QRS complex.
- Constant PR interval from beat to beat.
- QRS is often narrow unless there is coexisting bundle branch block or more distal conduction disease.
- No dropped QRS complexes.
⚠️ Clinical significance
- Usually benign, particularly in asymptomatic younger patients or athletes.
- May be a marker of increased vagal tone, medication effect, or underlying conduction system disease.
- Marked PR prolongation can occasionally cause symptoms such as fatigue, dizziness, or reduced exercise tolerance because atrial contraction occurs too early relative to ventricular filling.
- It may coexist with other conduction abnormalities and, in some settings, can progress to more advanced AV block.
🦠 Causes
- Normal variant.
- High vagal tone (for example athletes, sleep).
- Drugs: beta-blockers, verapamil, diltiazem, digoxin, amiodarone, some antiarrhythmics.
- Ischaemic heart disease or acute myocardial infarction.
- Myocarditis.
- Degenerative conduction system disease and age-related fibrosis.
- Electrolyte disturbance, especially potassium abnormalities.
- Infiltrative disease such as amyloidosis or sarcoidosis.
- Infective/inflammatory causes such as Lyme disease or diphtheria.
- Structural heart disease, congenital heart disease, or post-cardiac surgery.
- Aortic root abscess in infective endocarditis.
- Rheumatic fever (less common in UK practice).
🩺 Symptoms and examination
- Most patients are asymptomatic.
- Ask about presyncope, syncope, dizziness, chest pain, breathlessness, palpitations, and exercise intolerance.
- Review for recent infection, myocarditis symptoms, tick exposure, or drug toxicity.
- Check pulse, blood pressure, signs of heart failure, and features of systemic disease if relevant.
🔎 Investigations
- 12-lead ECG to confirm PR prolongation and look for other conduction abnormalities.
- Medication review is essential.
- U&Es, including potassium, calcium, and renal function if clinically indicated.
- TFTs if thyroid disease is suspected.
- Troponin if chest pain, myocardial infarction, or myocarditis is suspected.
- Inflammatory markers or infection screen if myocarditis/endocarditis is a concern.
- Echocardiography if structural heart disease is suspected.
- Ambulatory ECG monitoring if symptoms suggest intermittent higher-grade block or another arrhythmia.
💊 Management
- No specific treatment is needed for most asymptomatic patients.
- Correct reversible causes such as electrolyte disturbance or medication effect.
- Review rate-limiting drugs if the PR interval is markedly prolonged or the patient is symptomatic.
- Treat the underlying cause if present, for example ischaemia, myocarditis, Lyme disease, or infiltrative disease.
- If there are symptoms, syncope, very marked PR prolongation, broad QRS, or suspicion of more distal conduction disease, seek senior or cardiology review.
- Pacing is not usually required for isolated first-degree AV block, but may be considered in selected symptomatic patients with significant conduction delay.
🚑 When to worry
- Syncope or presyncope.
- Chest pain or suspected acute coronary syndrome.
- New conduction abnormality in the context of infective endocarditis, myocarditis, or post-procedure complications.
- Very prolonged PR interval with symptoms.
- Associated bundle branch block, bradycardia, or progression toward higher-grade AV block.
📝 Key exam points
- First-degree AV block = prolonged PR interval + no dropped beats.
- It is usually due to AV nodal delay.
- Common causes include high vagal tone, drugs, ischaemia, and structural/conduction system disease.
- Most cases are benign and need no treatment.
- Always think about the clinical context: symptoms, acute illness, medication effects, and whether there are other ECG abnormalities.
🖼️ Example ECGs