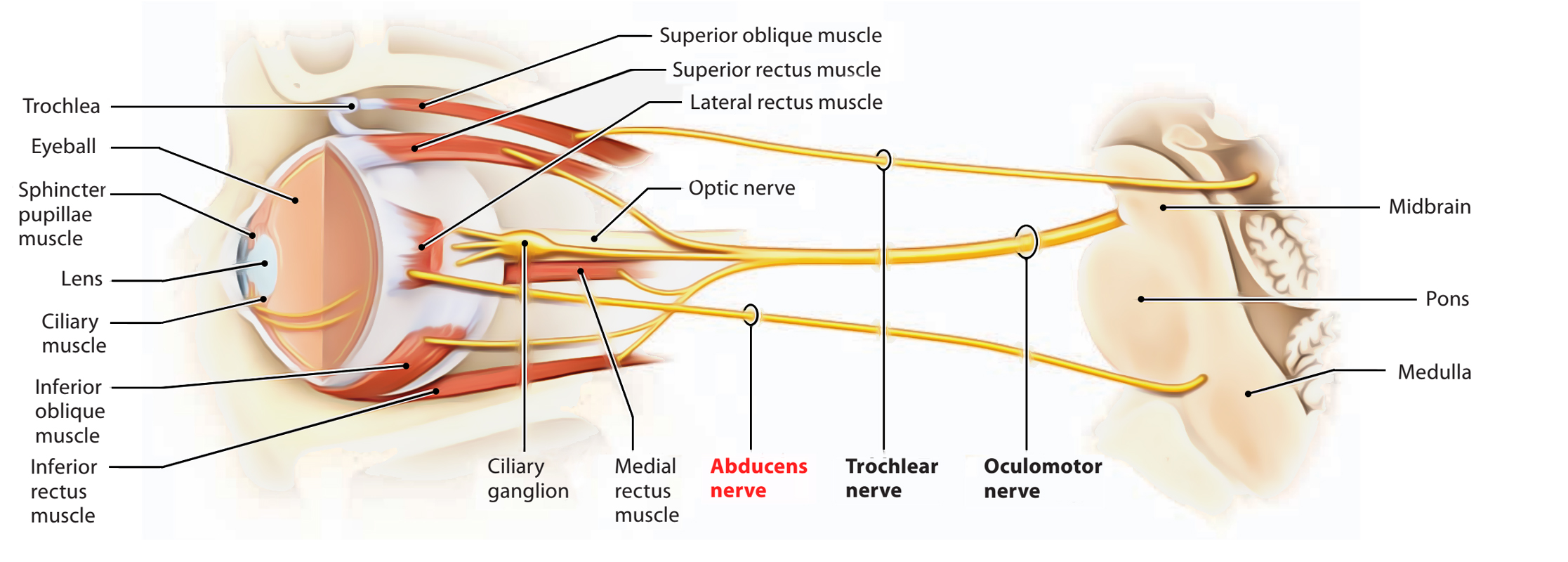
The oculomotor nerve (cranial nerve III) is responsible for most eye movements, pupil constriction, and maintaining an open eyelid. It can be incomplete and progressive until there is complete ptosis and complete weakness of the involved extraocular muscles to that eye is down and out.
A third nerve palsy produces ptosis 👁️, “down and out” eye deviation, diplopia, and possibly a dilated pupil depending on parasympathetic involvement. The key clinical discriminator is pupil involvement: compressive lesions (e.g. aneurysm) tend to affect superficial parasympathetic fibres early, whereas microvascular ischaemia often spares the pupil. Always consider this a potential neurosurgical emergency until aneurysm is excluded.
| Cause 🧩 | Typical Features 🔍 | Immediate Management 🚑 | Definitive / Ongoing Management 🏥 |
| Posterior communicating artery aneurysm 🩸 | Painful palsy, dilated non-reactive pupil, acute onset | Urgent CT angiography ± neurosurgical referral | Endovascular coiling or surgical clipping |
| Microvascular ischaemia (diabetes, hypertension) 🩺 | Pupil-sparing palsy, vascular risk factors | Exclude aneurysm if atypical; glucose/BP control | Usually resolves in 6–12 weeks; risk factor optimisation |
| Cavernous sinus pathology (thrombosis, tumour) 🧠 | Multiple cranial nerve deficits (III, IV, V1, V2, VI), proptosis | Urgent MRI ± MRV | Treat underlying cause (antibiotics, anticoagulation, oncology) |
| Brainstem infarction 🧠 | Associated long-tract signs (contralateral weakness) | Stroke pathway activation | Secondary stroke prevention |
| Trauma 🚗 | History of head injury | Urgent CT head | Neurosurgical management if required |
| Raised intracranial pressure ⚠️ | Bilateral or progressive palsy; reduced consciousness | Emergency neuroimaging | Treat cause (mass lesion, hydrocephalus) |
| Tumours 🎗️ | Progressive symptoms; may involve multiple nerves | MRI brain/orbits | Oncology / neurosurgical management |
| Inflammatory / demyelinating (e.g. MS) 🔥 | Young patient; other neurological deficits | MRI brain with contrast | Steroids if inflammatory; disease-modifying therapy |
| Myasthenia gravis 💪 | Fluctuating ptosis/diplopia; pupils normal | Check AChR antibodies; consider edrophonium/ice test | Pyridostigmine ± immunosuppression |
| Ophthalmoplegic migraine 🌩️ | Recurrent headache + transient palsy | Exclude structural causes | Supportive ± migraine prophylaxis |
Any acute third nerve palsy with a dilated pupil is an aneurysm until proven otherwise. Pain increases suspicion of compressive pathology. In older patients with vascular risk factors and a pupil-sparing palsy, microvascular ischaemia is common but still warrants imaging if atypical or incomplete. Early neuroimaging (CTA or MRA) is the cornerstone of safe practice.