
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Bites and stings
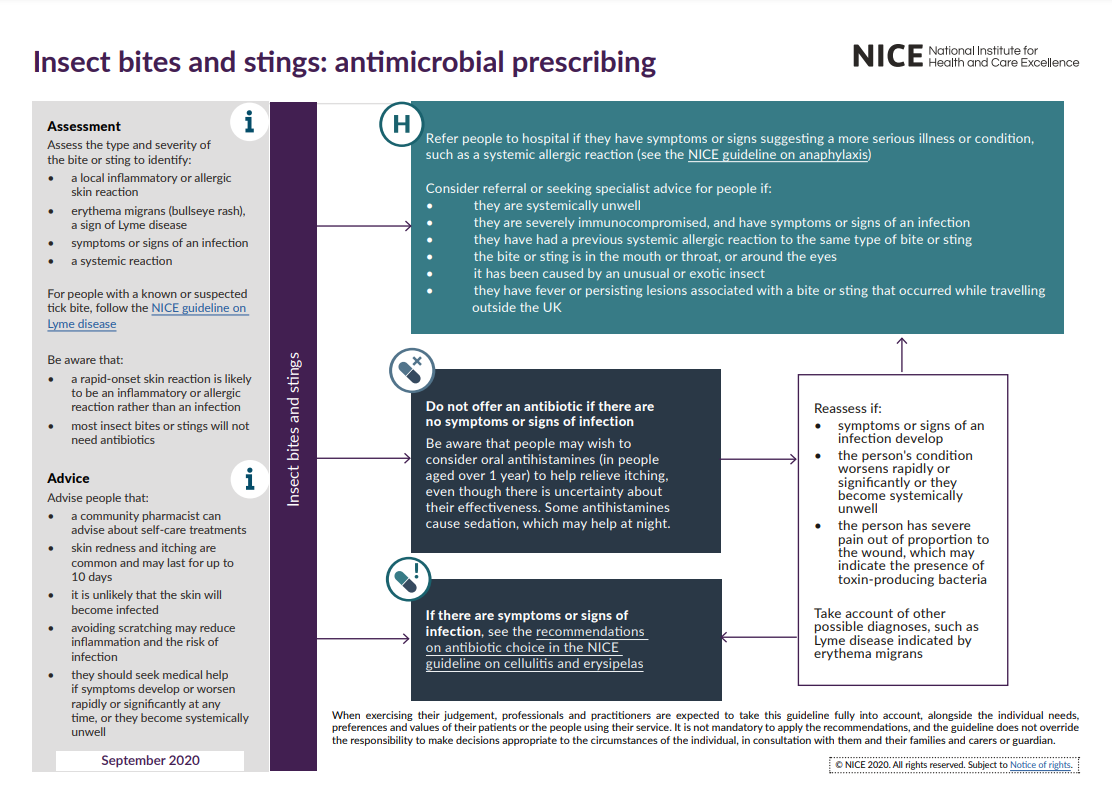
🩺 Bites and stings are a common reason for presentation to primary care, urgent care, and emergency departments in the UK. While many are self-limiting, some carry risks of serious infection, anaphylaxis, or zoonotic disease. ⚖️ NICE CKS guidance provides a framework for safe, evidence-based management in both adults and children.
💡 Key principle: Always assess for systemic involvement (airway compromise, widespread allergic reaction, sepsis) and local complications (infection, deep tissue injury, tissue necrosis).
🧪 General Approach
- 🔎 History: Type of bite/sting, time of onset, environment (UK vs abroad), systemic symptoms (fever, rash, SOB, collapse).
- 👀 Examination: Local wound (size, depth, discharge, foreign body), lymphadenopathy, systemic features.
- 🧾 Investigations (if severe/systemic): FBC, CRP, blood cultures, wound swab, U&E/LFTs if septic, Lyme serology (if tick + systemic).
- 💉 Immediate priorities: ABCDE approach, airway protection in suspected anaphylaxis, haemostasis, pain relief.
- 💊 Prophylaxis checks: Tetanus, rabies (if from endemic regions), hepatitis B (human bites).
🦟 Bites and Stings – Clinical Presentation & Management
- 🐝 Insect Bites/Stings (bees, wasps, mosquitoes)
- Clinical: Local itching, erythema, swelling; may cause anaphylaxis 🚨.
- Management:
- Mild ➝ ❄️ cold compress, non-sedating antihistamines, topical steroids
- Secondary infection ➝ oral antibiotics (flucloxacillin/clarithromycin)
- Anaphylaxis ➝ 🚑 IM adrenaline 500 mcg (adult) / 150–300 mcg (child) + O2, IV fluids, antihistamines, steroids
- Prevention ➝ repellents, protective clothing, avoidance advice
- 🕷️ Tick Bites
- Clinical: Local redness; risk of Lyme disease ➝ erythema migrans (target rash), flu-like illness, neurological/arthritic features later.
- Management:
- Careful removal with fine tweezers (close to skin, steady pull)
- Do not burn/suffocate the tick ❌
- If erythema migrans ➝ treat empirically (doxycycline 100 mg BD 21 days; amoxicillin in pregnancy/children)
- 🧑 Human Bites
- Clinical: Puncture/tearing wounds; high risk of infection (Eikenella, anaerobes).
- Management:
- Immediate irrigation, wound exploration, remove debris
- Prophylactic antibiotics ➝ co-amoxiclav 7 days
- Consider HIV/hepatitis B exposure prophylaxis if high-risk
- Tetanus vaccination if needed
- Escalate to IV antibiotics if cellulitis/sepsis
- 🐶 Animal Bites (dog, cat)
- Clinical: Dogs cause crush injuries; cats cause deep puncture wounds (→ Pasteurella multocida risk).
- Management:
- Thorough cleaning ± surgical debridement
- Antibiotics ➝ co-amoxiclav 7 days
- Tetanus update
- Rabies prophylaxis if animal from high-risk area 🌍
- 🕸️ Spider Bites
- Clinical: Local pain, erythema, swelling. Rare systemic ➝ cramps, abdominal pain.
- Management:
- Mild ➝ cold compress, analgesia
- Severe/systemic ➝ admit, supportive care ± antivenom
- 🌊 Jellyfish Stings
- Clinical: Burning pain, linear welts. Rare systemic ➝ arrhythmias, respiratory compromise.
- Management:
- Rinse with seawater (❌ not fresh water)
- Hot water immersion (40–45°C, 20–30 mins) to inactivate venom
- Systemic involvement ➝ emergency care
Special Considerations
- 👶 Children: More prone to systemic reactions and severe swelling. Always use weight-based dosing for antihistamines/antibiotics.
- 🤰 Pregnancy: Avoid doxycycline (tick bites) – use amoxicillin. Always consider maternal-fetal safety.
- 🧓 Immunocompromised: Higher risk of infection and poor healing ➝ lower threshold for IV antibiotics & admission.
- 🌍 Travel-related: Consider exotic infections (rabies, leishmaniasis, malaria, dengue). Always take a travel history.
Red Flags 🚩
- Rapidly spreading erythema, cellulitis, systemic upset → sepsis pathway.
- Signs of anaphylaxis (airway obstruction, wheeze, hypotension, collapse).
- Bites near critical structures (face, hands, genitals, joints) → higher complication risk.
- Deep puncture wounds (cats, humans) → very high infection risk.
Summary
🌟 Clinical takeaway: Most insect bites are benign, but human and cat bites, tick bites, and systemic allergic reactions require urgent recognition and early treatment. Always check tetanus & rabies status, and never miss anaphylaxis 🚨.
References
- NICE CKS: Insect bites & stings
- NICE CKS: Human bites
- NICE CKS: Animal bites
- UKHSA: Lyme disease guidance
🧾 Clinical Case Examples
Case 1 – Wasp sting anaphylaxis 🚑
A 40-year-old man is stung on the arm while gardening. Within 10 minutes he develops urticaria, lip swelling, stridor, and hypotension.
👉 Diagnosis: Anaphylaxis secondary to wasp sting.
👉 Management: IM adrenaline 500 mcg (1:1000), oxygen, IV fluids, admit for observation. Prescribe adrenaline auto-injector on discharge.
Case 2 – Infected cat bite 🐱
A 65-year-old woman presents 24 h after a cat bite to her hand. It is swollen, erythematous, and very tender. She is febrile (38.5 °C).
👉 Diagnosis: Cellulitis from Pasteurella multocida.
👉 Management: Wound cleaning, co-amoxiclav 7 days, IV antibiotics if deteriorating. Check tetanus status.
Case 3 – Tick bite with erythema migrans 🕷️
A 12-year-old boy returns from a camping trip in the New Forest. Ten days later he develops a circular expanding red rash with central clearing on his thigh, plus malaise.
👉 Diagnosis: Lyme disease (early).
👉 Management: Doxycycline 21 days (or amoxicillin if <12 y or pregnant).
Case 4 – Human bite in A&E 👊
A 19-year-old man is punched in the mouth during a fight, sustaining a “clenched fist” injury over the 3rd MCP joint. The wound is punctured and swollen.
👉 Diagnosis: Human bite with high infection risk (Eikenella, anaerobes).
👉 Management: Urgent wound irrigation, exploration, co-amoxiclav 7 days, hand surgery referral if joint involved.
Case 5 – Jellyfish sting abroad 🌊
A 25-year-old holidaymaker in Australia presents with burning pain and linear red welts after swimming. He is in distress but haemodynamically stable.
👉 Diagnosis: Jellyfish sting.
👉 Management: Rinse with seawater, hot water immersion 40–45 °C for 20 min, analgesia. Admit if systemic features (arrhythmia, respiratory compromise).
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery